

Alessandra Juliana de Carvalho
DOI: 10.17545/eOftalmo/2025.0017
Este artigo pertence à Edição Especial Intervenções Estratégicas em Reabilitação: Estimulação Precoce à Autonomia Funcional
ABSTRACT
PURPOSE: To synthesize current knowledge on the adaptation of the home environment for people with low vision and its impact on the performance of daily activities.
METHODS: This narrative review focuses on recent literature on lighting, contrast, spatial organization, home safety, and assistive technologies in low vision, in the context of the International Classification of Functioning, Disability and Health and of the person-environment-occupation-performance model.
RESULTS: Evidence indicates that environmental interventions in the home improve functional performance, safety, autonomy, and quality of life. Strategies such as optimizing lighting, controlling glare, using color contrast, organizing space, preventing falls, and incorporating assistive technologies exhibit consistent benefits and a good cost-effectiveness ratio.
CONCLUSION: The adaptation of the home environment should be considered the central axis of the rehabilitation for low vision. Personalized home interventions are fundamental to increasing social participation, safety, and functional independence.
Keywords: Low vision; Environment adaptation; Activities of daily living; Lighting; Accessibility.
RESUMO
OBJETIVO: Sintetizar o conhecimento atual sobre a adaptação do ambiente doméstico para pessoas com baixa visão e seu impacto no desempenho das atividades de vida diária.
MÉTODOS: Revisão narrativa da literatura recente sobre iluminação, contraste, organização espacial, segurança domiciliar e tecnologias assistivas aplicadas à baixa visão, articulada com a Classificação Internacional de Funcionalidade, Incapacidade e Saúde e o modelo pessoa–ambiente–ocupação–desempenho.
RESULTADOS: Evidências indicam que intervenções ambientais no domicílio melhoram o desempenho funcional, a segurança, a autonomia e a qualidade de vida. Estratégias como otimização da iluminação, controle do ofuscamento, uso de contraste cromático, organização espacial, prevenção de quedas e incorporação de tecnologias assistivas apresentam benefícios consistentes e boa relação custo-efetividade.
CONCLUSÃO: A adaptação do ambiente doméstico deve ser considerada eixo central da reabilitação em baixa visão. Intervenções domiciliares personalizadas são fundamentais para ampliar a participação social, a segurança e a independência funcional.
Palavras-chave: Baixa visão; Adaptação ambiental; Atividades de vida diária; Iluminação; Acessibilidade.
INTRODUCTION
Low vision is a major public health problem that significantly impacts functionality, independence, and quality of life. The World Health Organization estimates that hundreds of millions of people live with moderate or severe visual impairment, with a higher prevalence among older adults and in middle- and low-income countries1. In Brazil, an aging population and the growing prevalence of chronic eye diseases have led to the need for effective visual rehabilitation strategies.
Historically, visual rehabilitation has focused on clinical interventions and the use of optical devices. However, the notion that the home environment plays a decisive role in the performance of daily activities has been consolidated in recent decades2. In this context, adapting the home environment emerges as an essential strategy to reduce barriers to clinical management, promote safety, and preserve functional independence.
The International Classification of Functioning, Disability and Health (ICF) proposes that disability results from the interaction between the individual's health condition and contextual factors, including the physical environment3. Thus, modifying the home environment is not just a complementary measure but also an integral part of the rehabilitation process.
This article presents an up-to-date synthesis of current knowledge on adapting the home environment for people with low vision. Theoretical foundations, scientific evidence, and practical implications for the ophthalmic community have been discussed.
DEVELOPMENT
Theoretical foundation: person-environment-occupation-performance model and ICF
The person-environment-occupation-performance (PEOP) model proposes that occupational performance results from the dynamic interaction between individual characteristics, activity demands, and environmental factors4. In the context of low vision, although sensory limitations often cannot be reversed, the environment can be modified to reduce the gap between inability and functional demand.
As a complement to the PEOP, the ICF reinforces that environmental factors can act as barriers or facilitators of performance3. Thus, interventions in the home environment are a key strategy for optimizing functionality, participation, and quality of life of individuals with low vision.
Recent studies have shown that modifications to the home environment improve the performance of daily activities, reduce the risk of falls, and increase confidence in performing daily tasks5,6.
Lighting and glare control
Lighting is one of the most critical elements in adapting the home environment for people with low vision. Inadequate levels of lighting compromise the performance of tasks such as preparing food, reading labels, personal hygiene, and handling medication7.
A combination of ambient lighting and task lighting is recommended, with adjustable intensity and even distribution of light. Lamps with diffusers, indirect lighting, and translucent curtains help control glare, especially in the case of individuals with cataracts, age-related macular degeneration, and retinopathies (Figure 1)8.

The modifications must be individualized because the kind of light needed varies according to the ocular disease, age, and the nature of the task performed9.
Color contrast, colors, and signage
Reduced sensitivity to contrast is common in several eye diseases and directly affects the identification of objects and spatial boundaries (Figure 2)10.

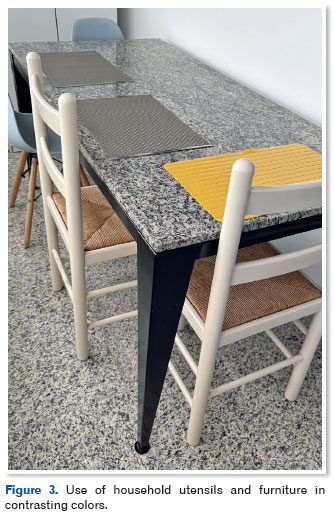
The strategic use of color contrast between surfaces, objects, and backgrounds facilitates visual perception and helps avoid mistakes during daily activities. Examples include the use of utensils and furniture in contrasting colors and the visual separation of functional boundaries (Figure 3).
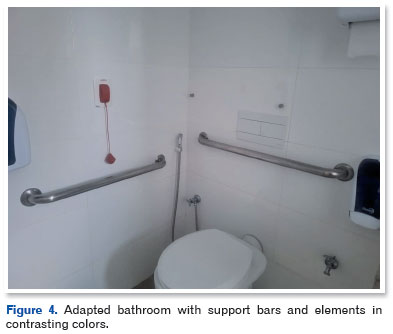
In the bathroom, using different colors for the toilet, sink, and wall contributes significantly to safety and spatial orientation (Figures 4, 5, and 6)11.


The combination of tactile and visual signage increases accessibility and promotes functional independence, particularly in cases of progressive visual loss (Figure 7)5.
Spatial organization and routine structuring
Disorganized environments increase cognitive load, make it difficult to locate objects, and increase the risk of accidents6. Maintaining everyday items in the same place, reducing excess, and simplifying the space are fundamental strategies.
Predictability of the environment reduces exclusive dependence on visual information and improves functional efficiency. The active participation of the individual in the reorganization process is important for adherence and the success of the adaptations2.
Home safety and prevention of falls
Visual impairment is a known risk factor for falls, especially among older adults7. Essential measures include removing loose carpets, using non-slip flooring, installing handrails and support bars, improving lighting in circulation areas, and properly marking steps and uneven surfaces.
Home interventions focused on preventing falls lead to greater adherence and a positive impact on safety and confidence in performing daily activities5.
Assistive technologies in home settings
Assistive technologies range from traditional optical devices to digital solutions such as reading applications, object recognition, and voice command assistants12. The effectiveness of these resources depends on adequate training and their integration into everyday activities and complementary environmental modifications2.
Person- and family-centered approach
The adaptation of the environment must take into account emotional, cultural, and social aspects. Visual loss is often associated with insecurity and fear, warranting a sensitive and collaborative management approach5. Active participation of the affected individual and involvement of the family favor functional independence and adherence to interventions6.
DISCUSSION
Adapting the home environment for people with low vision represents a paradigm shift in visual rehabilitation, with the focus no longer solely on clinical treatment but also on functionality in real-life situations.
Evidence indicates that home environment interventions result in significant gains in autonomy, safety, and quality of life5,6. Strategies such as improving lighting, using color contrast, and preventing falls have shown consistent effectiveness and applicability in different contexts.
In conclusion, adapting the home environment is an essential strategy for promoting autonomy, safety, and participation in daily activities among people with low vision. This strategy must be understood as the central axis of visual rehabilitation as it contributes to the dignity, social participation, and the full exercise of citizenship of the affected individuals.
REFERENCES
1. World Health Organization. World report on vision. Geneva: WHO; 2021. Disponível em: https://www.who.int/publications/i/item/world-report-on-vision
2. Markowitz J. Principles of modernlow vision rehabilitation. Can J. Ophthalmol. 2006;41(3):289-312.
3. World Health Organization. ICF. Geneva: WHO; 2001. Disponível em: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health
4. Law M, Cooper B, Strong S, Stewart D, Rigby P, Lettes L. The person-environment-occupation model: a transactive approach to occupational performance. Can J Occup Ther. 1996;63(1):9-23.
5. Lamoureux EL, Pallant JF, Pesudovs K, Rees G, Hassell JB, Keeffe JE. The effectiveness of low-vision rehabilitation on participation in daily living and quality of life. Invest Ophthalmol Vis Sci. 2007;48(4):1476-1482.
6. Owsley C, McGwin G, Sloane ME, Stalvey BT, Wells J. Timed instrumental activities of daily living tasks: relationship to visual function in older adults. Optom Vis Sci. 2001;78(5):350-359.
7. Owsley C, McGwin G Jr. Vision impairment and driving. Surv Ophthalmol. 1999;43(6):535-550.
8. Boyce PR. Human factors in lighting. 3rd ed. Boca Raton: CRC Press; 2014.
9. Owsley C. Aging and vision. Vision Res. 2011;51(13):1610-1622.
10. Pelli DG, Bex PJ. Pelli DG, Bex PJ. Measuring contrast sensitivity. Vision Res. 2013 Sep 20;90:10-4.
11. Szlyk JP, Seiple W, Laderman DJ, Kelsch R, Ho K, McMahon T. Use of bioptic amorphic lenses to expand the visual field in patients with peripheral loss. Optom Vis Sci. 1998;75(7):518-24.
12. Virgili G, Acosta R, Bentley SA, Giacomelli G, Allcock C, Evans JR. Reading aids for adults with low vision. Cochrane Database Syst Rev. 2018 Apr 17;4(4):CD003303.
| AUTHOR INFORMATION |
|
 |
» Alessandra Juliana de Carvalho https://orcid.org/0000-0001-6247-3653 http://lattes.cnpq.br/5766780157438980 |
Funding: The author declares no funding.
Conflicts of interest: The author declares no conflicts of interest.
Received on:
January 20, 2026.
Accepted on:
February 2, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket