

Guilherme B. Guedes
DOI: 10.17545/eOftalmo/2025.0002
Este artigo pertence à Edição Especial SLT no Glaucoma: Da Prática Clínica à Perspectiva de Implementação no SUS
ABSTRACT
Selective laser trabeculoplasty has been established as a safe and effective treatment for controlling intraocular pressure in open-angle glaucoma and ocular hypertension. It evolved from a rescue treatment to a first-line option. The technique offers superior pressure stability to initial monotherapy and preserves the quality of life and the health of the ocular surface. The procedure is especially indicated in cases of ocular hypertension and for the treatment of initial to moderate open-angle glaucoma, with high baseline intraocular pressure being the strongest and most reliable predictor of treatment success. Because of its absence of coagulative damage, selective laser trabeculoplasty is repeatable, with studies indicating that the duration of the effect of retreatment can even exceed that of the initial application. However, this procedure is contraindicated in cases with active inflammation, neovascularization, and closed angle. Selective laser trabeculoplasty has a robust safety profile with rare serious complications. Thus, the technique serves as a strategic tool to reduce polypharmacy and postpone invasive surgical interventions.
Keywords: Selective laser trabeculoplasty; Openangle glaucoma; Intraocular pressure; LiGHT trial; First-line treatment; Repeatability; Pressure fluctuation.
RESUMO
A trabeculoplastia seletiva à laser consolidou-se como uma terapia segura e eficaz para o controle da pressão intraocular no glaucoma de ângulo aberto e hipertensão ocular. Evoluindo de um tratamento de resgate para uma opção de primeira linha. A técnica oferece estabilidade pressórica superior à monoterapia inicial, preservando a qualidade de vida e a saúde da superfície ocular. O procedimento é especialmente indicado em casos de hipertensão ocular com indicação de tratamento e glaucoma de ângulo aberto inicial a moderado, tendo a pressão intraocular basal elevada como o preditor de sucesso mais forte e fiável. Devido ao seu mecanismo não destrutivo, a trabeculoplastia seletiva à laser é repetível, com estudos indicando que a duração do efeito do retratamento pode, inclusive, superar a da aplicação inicial. É contraindicada em situações de inflamação ativa, neovascularização ou ângulo fechado. A trabeculoplastia seletiva à laser apresenta um perfil de segurança robusto com raras complicações graves. Assim, a técnica atua como uma ferramenta estratégica para reduzir a polifarmácia e postergar intervenções cirúrgicas invasivas.
Palavras-chave: Trabeculoplastia seletiva à laser; Glaucoma de ângulo aberto; Pressão intraocular; LiGHT trial; Primeira linha de tratamento; Repetibilidade; Flutuação pressórica.
INTRODUCTION
Over the last two decades, selective laser trabeculoplasty (SLT) has been established as an effective, safe, and reproducible treatment modality for reducing intraocular pressure (IOP) in patients with open-angle glaucoma and ocular hypertension (OHT). Its clinical role has evolved from a "rescue" treatment for eyes, for which maximum tolerated clinical treatment failed, to a fully indicated initial treatment option in well-defined scenarios, backed by robust evidence from randomized clinical trials, long-term studies, and meta-analyses. Based on the evidence currently available, the clinical indications for SLT can be systematized as described below.
INDICATIONS, PREDICTORS, AND CONTRAINDICATIONS
Indication by type of glaucoma
The efficacy of SLT varies according to the pathophysiology of each type of glaucoma. Previous studies highlight the following specific indications:
• Ocular hypertension (OHT): Patients with a high IOP but no glaucomatous lesion are excellent candidates. Early treatment with SLT can delay or prevent the need for medication or surgery and help maintain quality of life and an intact ocular surface.
• Primary open-angle glaucoma (POAG): This is the gold standard indication. The LiGHT1 study confirmed that SLT is highly effective as an initial treatment in individuals with POAG as this procedure provides stable pressure control without the common fluctuations observed with eye drops.
• Pigmentary glaucoma: This subtype is particularly responsive to SLT because the laser specifically targets melanin (pigment) in the trabecular meshwork. The large amount of pigment leads to greater energy absorption.
🞅 Clinical Note: Caution is advised. Lower energy than usual should be used to avoid hypertensive peaks or excessive post-laser inflammation.
• Pseudoexfoliative glaucoma (PEX): Patients with PEX tend to have higher baseline IOP and, consequently, have more dramatic and expressive pressure reductions with SLT.
🞅 Caveat: The literature points out that, despite the excellent initial response to the laser, its effect can "fail" or diminish earlier in this type of glaucoma than in POAG, thereby requiring closer monitoring2.
• Normal tension glaucoma (NTG): SLT is indicated and effective in NTG, but the absolute reduction in IOP (mmHg) tends to be lower than in high-pressure glaucoma (due to the "floor effect"). The greatest benefit in this group is the reduction in day/night fluctuations in IOP, as SLT stabilizes pressure and reduces peaks that occur outside of office hours3.
• Steroid-induced glaucoma: Although this type of glaucoma is less addressed in large trials, it is an excellent indication pathophysiologically, because the change in the trabecular meshwork caused by corticosteroids is often reversed or improved by SLT4,5.
Indication by clinical scenario
The clinical versatility of SLT allows it to be strategically integrated into different clinical situations. It is currently indicated in different practical scenarios with the aim of personalizing treatment to the specific needs of each patient, as discussed below (Figure 1):
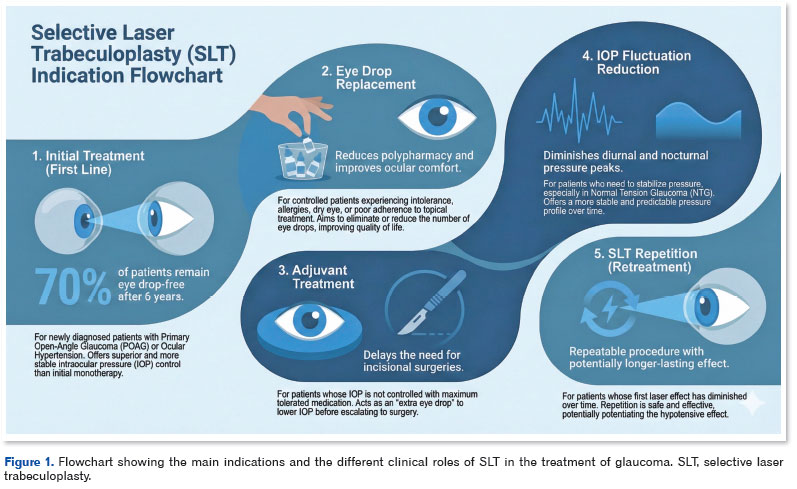
1. As initial treatment (first-line)
The indication of SLT as first-line treatment represents the most significant paradigm shift in recent years, supported mainly by the LiGHT Trial1. In this scenario, SLT is offered to newly diagnosed patients (treatment-naive) with initial to moderate POAG or OHT, before eye drops are prescribed. Studies show that this approach is not only safe but also provides better and more stable control of IOP than initial monotherapy with prostaglandins6,7. After 6 years, around 70% of patients treated with SLT remained without the need for eye drops to achieve the target IOP6. In addition to its clinical efficacy, this indication stands out for its favorable cost-effectiveness ratio and for preserving quality of life by preventing early adverse effects on the ocular surface associated with the chronic use of eye drops.
2. For eye drop replacement in controlled glaucoma
This indication is essential for patients who, although controlled, suffer from the burden of topical treatment. SLT is used in this case with the aim of reducing polypharmacy (removing one or more medications) or eliminating the need for eye drops. SLT is indicated for patients with drug intolerance, allergies to medications or preservatives, dry eye exacerbated by eye drops, or physical and cognitive difficulties that compromise adherence (forgetfulness or difficulty applying eye drops). The real-world study on SLT conducted in Brazil8 reinforces that the average reduction in medication (from 1.8 to 1.4 per patient) is a common and desirable outcome that improves ocular comfort and facilitates long-term adherence to treatment9.
3. Adjuvant to clinical treatment
When IOP is not adequately controlled with the use of the maximum tolerated medication alone, SLT serves as an additive or adjuvant therapy. In this context, the laser acts as an "extra eye drop" that helps lower IOP to safe levels and postpone the need for incisional surgery (such as trabeculectomy). Although the absolute reduction in IOP may be lower in the eyes of patients who already use multiple eye drops (due to less outflow and possible chronic changes in the trabecular meshwork), SLT still offers the possibility to improve IOP without adding more complexity to the patient's dosage regimen. It is a valid rescue attempt before escalating to the operating room.
🞅 Note: In this situation, the chance of a response to the laser is significantly lower compared to patients with a healthier trabecular meshwork. Therefore, it is essential to verify beforehand the possibility of operating post-SLT.
4. Reducing fluctuations in intraocular pressure
Previous studies have reported that SLT acts as a powerful IOP stabilizer by mitigating circadian variations and long-term oscillations. In the context of 24-h fluctuations, the randomized clinical trial by Kiddee and Atthavuttisilp3 provided comparative data showing that SLT is as effective as prostaglandins (Travoprost) in reducing mean IOP in patients with POAG, but stands out specifically in normal tension glaucoma (NTG) in which SLT had higher success rates than eye drops in reducing circadian fluctuation. These findings were in line with those of Pillunat et al.10, who confirmed the ability of SLT to "flatten" the daily curve and reduce nocturnal peaks in already medicated eyes.
In addition, from a long-term perspective, real-life data from Cordeiro et al.11 show an extension of this benefit to long-term fluctuation (inter-visit variability), thus proving that the procedure offers a more predictable and stable pressure profile over 24 months.
5. Repeat SLT (retreatment)
SLT is a repeatable procedure due to its absence of coagulative damage that preserves the architecture of the trabecular meshwork. Repetition is indicated when the effect of the first laser diminishes over time (which is to be expected after a few years). The LiGHT Trial protocol12 allowed retreatment after two months, thus demonstrating that SLT repetition is safe and effective, often achieving IOP reductions similar to those obtained after the initial treatment. Garg and Gazzard2 suggest that if the first treatment led to a good outcome (duration of effect > 6 months), retreatment has a high probability of success.
In terms of clinical results, retreatment was not only effective but also had an additive effect and greater durability. In the 6-year follow-up of the LiGHT study, 70.7% of patients had their IOP under control without the need for eye drops. Among them, 34.4% required two applications of SLT and 10% required three or more treatments6. Although the absolute drop in pressure (mmHg) was lower in retreatment due to a lower baseline IOP (ceiling effect), the reduction in adjusted IOP was statistically higher than in the initial treatment, which suggests potentiation of the hypotensive effect.
In the LiGHT12 and LiGHT-China13 studies, a favorable clinical pattern was observed where the duration of the effect of the second treatment (repetition) tended to exceed that of the initial treatment in eyes that had failed the first laser. The LiGHT study showed that, for the same patients, the duration of the effect of the repeat laser procedure was significantly longer than that of the first procedure (extending beyond 18 months in retreatment versus approximately six months in the initial treatment). This trend was corroborated by data from the LiGHT-China study13, which concluded that the second SLT not only has the capacity to further reduce IOP but also potentially has a longer-lasting effect than the first SLT that failed, which suggests that the temporal efficacy of the laser does not decrease with repetition but is rather enhanced12,13.
Predictive factors for successful SLT
To maximize treatment efficacy and refine patient selection, it is essential to understand the clinical and anatomical variables that act as prognostic determinants of the response to SLT. The main factors identified are as follows:
• Baseline intraocular pressure (IOP): It is consistently the strongest and most reliable predictor of treatment success14-16. Statistical analyses in randomized clinical trials and cohort studies show the following positive correlation: the higher the preoperative IOP, the greater the absolute pressure reduction (in mmHg) tends to be. Eyes with clinical success have, on average, significantly higher basal pressure than those that fail treatment16.
• Pigmentation of the angle: The anatomy of the trabecular mesh plays an important role. It has been observed that eyes with a higher degree of angle pigmentation tend to have better success rates, because melanin acts as the target chromophore for absorbing laser energy16. However, related reviews warn that, despite the greater potential efficacy, these eyes require caution due to the increased risk of transient post-laser hypertensive peaks7.
• Stage of glaucoma: The severity of glaucomatous damage does not seem to be a factor that prevents laser treatment, although it does require different monitoring criteria. Studies have shown that SLT is safe and effective in both early and advanced stages, achieving success rates of 66% and 59% in the early and moderate/advanced glaucoma groups, respectively (considering an IOP reduction of >20% or medication reduction)17. However, in advanced glaucoma, the indication comes with a caution: although it is a tool for patients with moderately elevated IOP or under maximum medication, a significant proportion of them (18%) may require filtering surgery in the first year after the laser17.
• Demographic characteristics and type of glaucoma: Variables such as age and gender are not consistent predictors, with contradictory results. In terms of diagnosis, POAG and pseudoexfoliative glaucoma have been identified as having the most favorable responses7. The literature also suggests that previous chronic use of prostaglandin analogues can theoretically reduce the magnitude of the response to the laser, although this factor is not an impediment to treatment and there is no consensus in the literature2.
• Laser parameters and total energy: The influence of the energy used during the procedure is a point of technical discussion. Evidence from large trials suggests that greater total energy delivered during treatment (with full 360° application and a higher number of shots) may be associated with a higher likelihood of keeping the patient medication-free in the long term14. However, other studies have not found a simple linear correlation between accumulated energy and success, indicating that the biological response is variable16.
Contraindications to SLT
With regard to contraindications, it is essential to understand that the efficacy of SLT depends directly on its ability to remodel and increase the permeability of the trabecular meshwork. Therefore, in clinical situations where resistance to aqueous humor outflow is caused by pre-trabecular alterations (such as a closed iridocorneal angle, inflammatory or neovascular membranes covering the angle) or by post-trabecular alterations (such as increased episcleral venous pressure), the laser tends to have no effect. In addition to this pathophysiological limitation, contraindications are based on the inability to visualize the target structures or the presence of conditions that may be aggravated by the inflammatory mechanism of the procedure (Figure 2).
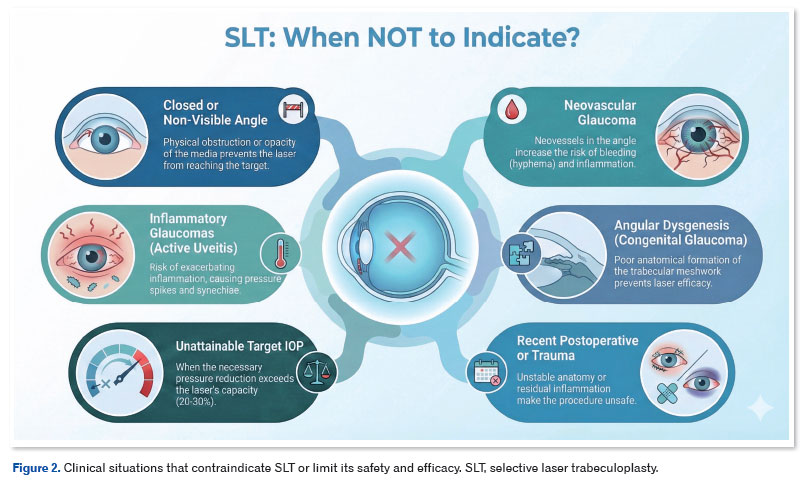
1. Closed-angle glaucoma
It is the classic contraindication. The trabecular meshwork is not visible on gonioscopy due to apposition or adherence of the iris (peripheral anterior synechia). Mechanical obstruction prevents the laser from reaching the trabeculae. Previous studies have reported the possibility of performing SLT in areas where the angle has become patent after peripheral iridotomy or phacoemulsification2,6.
2. Poor visualization of the angle and media opacities
It is the primary technical prerequisite. SLT requires the precise application of the laser to the trabecular meshwork; therefore, any condition that prevents this direct visualization makes treatment unfeasible. The leading underlying causes include significant corneal edema and corneal scarring (leukoma). If the surgeon cannot properly focus the aiming beam on the trabecular meshwork, the treatment cannot be performed safely and effectively18.
3. Inflammatory and uveitic glaucomas
The presence of active intraocular inflammation (uveitis) is an absolute contraindication. The mechanism of action of SLT involves the induction of a biological response mediated by cytokines and the recruitment of macrophages. Performing the procedure on an eye with active uveitis can dangerously exacerbate the inflammatory condition, leading to severe hypertensive spikes and the formation of synechiae2. Even in cases with quiescent uveitis, the indication should be made with extreme caution.
4. Neovascular glaucoma
The presence of neovessels in the iridocorneal angle contraindicates the procedure [2]. The fibrovascular membrane (pre-trabecular alteration) prevents the laser from directly accessing the trabecular meshwork, and furthermore, applying energy to these anomalous vessels entails a risk of hyphema and increased inflammation, without promoting a reduction in IOP.
5. Congenital glaucoma and goniodysgenesis
Patients with congenital or juvenile glaucoma, characterized by dysgenesis (malformation) of the angle, generally do not respond to SLT1,2. The structural anatomical alteration of the trabeculae in these cases prevents selective photothermolysis from exerting its tissue remodeling effect.
6. Recent surgery and trauma
A previous review mentions the relative contraindication in eyes with recent intraocular surgery or acute trauma, where the anatomy may be unstable or inflammation may still be present18. The LiGHT1 study excluded patients with previous intraocular surgery (with the exception of uncomplicated phacoemulsification performed more than three months previously) to ensure their safety.
7. Incompatibility with target IOP (insufficient hypotensive capacity)
Finally, we do not recommend SLT treatment when the tension reduction required to reach the target IOP exceeds the laser's statistical hypotensive capacity. Knowing that SLT provides, on average, a 20%–30% reduction in baseline pressure (equivalent to the effect of a prostaglandin)2,18, patients with very high IOP who need drastic reductions (for example, greater than 40% or 50%) to halt the progression of the disease are not ideal candidates for the laser. In these cases of severe dysregulation, insisting on SLT can delay surgery or more effective treatments, exposing the optic nerve to unnecessary risk.
3. Side effects and complications
SLT stands out for its robust safety profile, with an extremely low rate of serious complications compared to other glaucoma interventions. Adverse effects can be categorized into transient side effects (common) and serious complications (rare).
Transient side effects
The most common adverse event is a transient hypertensive peak (acute IOP rise) shortly after the procedure. The LiGHT1 study showed that these spikes are generally short-lived and self-limiting, resolving within 48 h, and rarely require intervention. In this study, six patients had an IOP spike of more than 5 mmHg out of 355 patients treated, an incidence of 1.7%. Another common side effect is a mild inflammatory reaction in the anterior chamber, manifested by cells or a flare, which is partly intrinsic to the laser's biological mechanism of action. Patients may also report mild eye discomfort, redness, and photophobia in the first few days2,14.
Serious complications
Complications that threaten vision are rare. A recent Finnish cohort study20 confirmed the rarity of serious events with SLT. In an analysis of 6,081 procedures (4,601 eyes), the incidence of complications was minimal, with only four cases of hyphema (0.07%) and six cases of corneal edema (0.1%), and only one event resulting in permanent refractive sequelae. However, some studies have highlighted specific cases of sustained IOP increase, peripheral anterior synechia formation, corneal edema, and refractive changes2,21.
4. Parameters
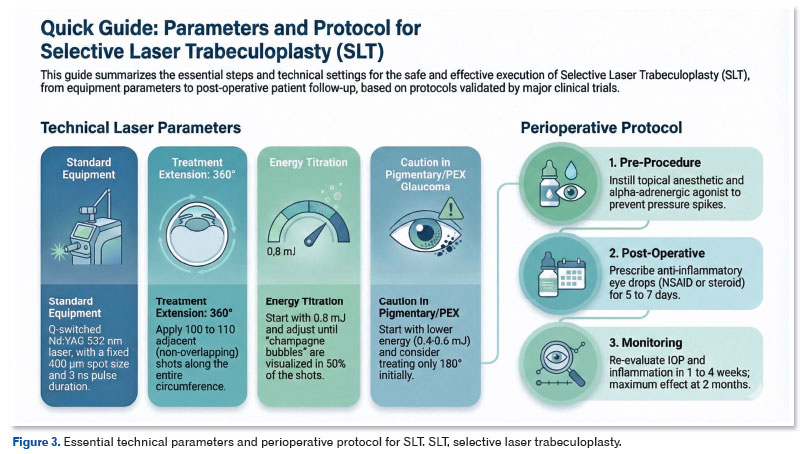
Based on the protocols validated by LiGHT23, large clinical trials and recent meta-analyses16,19, the recommended technical standardization for performing SLT is described below (Figure 3).
Equipment
SLT is performed using a 532 nm Q-switched Nd:YAG laser. The technical specifications to guarantee the principle of selective photothermolysis consist of a fixed spot size of 400 µm and an extremely short fixed pulse duration of 3 ns.
A specific goniolaser lens is used with methylcellulose or ophthalmic gel. The scleral spur is identified, and the pigmented trabecular meshwork is focused on (which should be in the center of the target area).
Extent of treatment (degrees and shots)
The current evidence consolidates the 360° application as the standard of excellence for first-line treatment and retreatment. The technical aim is to apply approximately 100 to 110 adjacent (non-overlapping) shots along the entire circumference of the iridocorneal angle.
In the article Efficacy of Repeat Selective Laser Trabeculoplasty - LiGHT Trial12, the protocol for repeat SLT remained similar to the initial treatment, consisting of applying the laser to 360° of the trabecular mesh with 100 to 110 shots. The main technical difference was the use of a significantly higher total energy in the second session compared to the first session (average of 100.5 mJ in retreatment versus 89.1 mJ in the initial one).
The treatment of pigmentary and pseudo-exfoliative glaucoma requires a precise adjustment of the parameters due to the hyperpigmentation of the trabecular meshwork, which drastically increases the absorption of laser energy. To ensure safety and avoid hypertensive peaks or severe inflammation, it is recommended to start with reduced energy levels (typically 0.4 to 0.6 mJ), and consider partial treatment of only 180° with 50 shots in the first session, titrating the power carefully to operate at the lower limit or slightly below the power that leads to the formation of microbubbles ("champagne bubbles"). And if necessary, the other 180° can be completed in a second session24. It is important to note which area of the angle is being treated in each session.
Energy Titration and "Champagne Bubbles"
Determining the ideal energy for each patient is a dynamic and personalized step, and can even vary from one quadrant to another quadrant of the same eye, as discussed below:
1. Initial energy: The laser is usually started with an energy of 0.8 mJ.
2. Adjustment (Titration): The energy is gradually increased or decreased by 0.1 mJ until small cavitation bubbles (described as "champagne bubbles") are visualized immediately after the shot.
3. Treatment energy: Traditional treatment uses energy that produces fine visible bubbles in at least half of the applications.
🞅 Note: In the LiGHT study, the energy used ranged from 0.3 to 1.4mJ.
🞅 Tip 1: Watch your focus during application, because if you lose focus, you may not see the bubbles.
🞅 Tip 2: We suggest always following the same pattern of application in the sequence of quadrants (for example, clockwise starting at the lower or lower/nasal/superior/temporal angle).
PERIOPERATIVE PROTOCOL
The perioperative approach to SLT is divided between immediate prophylaxis of tension spikes and modulation of the subsequent inflammatory response.
Pre-procedure preparation and prophylaxis
The established standard protocol requires the instillation of a topical anesthetic and of an alpha-adrenergic agonist immediately before or immediately after the procedure. This measure aims to prevent the occurrence of transient spikes in IOP, a common adverse event that results from the release of pigment debris and acute inflammation in the trabecular meshwork. It is not necessary to suspend the patient's usual hypotensive medication, which should be kept unchanged during the perioperative phase.
Post-operative anti-inflammatory regimen
Post-laser management aims to control patient discomfort while preserving the biological response of trabecular remodeling22. The classic protocol advocates the use of non-steroidal anti-inflammatory eye drops or steroids (such as prednisolone acetate) for a short period (for example, 3–4 times a day for 5–7 days).
• Monitoring: In addition to specific monitoring for signs of persistent corneal edema (especially in corneas with compromised endothelium), a re-evaluation appointment between one and four weeks after the procedure is recommended for all patients. The aim of this visit is to check the IOP to rule out late spikes or early failure, assess the level of inflammation in the anterior chamber, and confirm the resolution of any immediate symptoms. However, the maximum hypotensive effect should only be assessed and considered for therapeutic decisions around two months post-laser.
CLINICAL CASES
Case 1
Identification: Male, 47, executive.
Complaint: Asymptomatic, referred for elevated IOP on routine examination. No systemic comorbidities.
Ophthalmic examination:
• Biomicroscopy: Transparent cornea, deep anterior chamber, iris without particularities.
• Gonioscopy: Open angle (Shaffer Grade 4), trabecular pigmentation 2+/4+ (moderate).
• Pachymetry: 545 / 550 µm.
• Basal IOP (at 10 a.m.): 24 / 25 mmHg.
• Fundus of the Eye: Papillary excavation 0.6 × 0.6 with thinning of the inferior neuroretinal rim in both eyes.
• Optic Nerve OCT: Tapering of the RNFL in the temporal-inferior sector.
• Visual Field:
🞅 OD: MD: −2.8 dB. Early superior arcuate scotoma.
🞅 OS: MD: −1.3 dB. Normal.
Diagnosis: Initial POAG.
Management: Primary SLT was chosen as the first line of treatment (LiGHT Protocol).
• Justification: Based on the LiGHT1 study, SLT offers pressure control similar to that of prostaglandins but with better cost-effectiveness, guaranteed adherence, and preservation of the ocular surface.
• Procedure: SLT 360°, ~100 shots, energy titrated to 0.8 mJ, total energy 81.6 mJ.
• Outcome (6 months): IOP reduced to 17 mmHg AO (~30% reduction). Patient continues without using eye drops, only being monitored.
Case 1: The Ideal Candidate: Young patient, recent diagnosis, treatment-naive.
Case 2
Identification: Woman, 78, retired.
Complaint: "I can't apply so many eye drops and they're expensive." She reports frequent forgetfulness.
Background: Glaucoma for 15 years. Medications: Latanoprost + Timolol/Brimonidine twice/daily (3 drugs, 2 bottles).
Ophthalmic examination:
• Biomicroscopy: Early nuclear cataract.
• Gonioscopy: Open angle, 2/4+ pigmentation.
• Pachymetry: 498 µm AO (thin cornea - risk factor).
• IOP (no medication used that day): 19 / 18 mmHg. Target IOP <16 mmHg.
• Fundus of the Eye: Papillary excavation 0.75 × 0.8 with a lower notch in both eyes.
• Optic Nerve OCT: Diffuse thinning of the RNFL with severe localized loss in the inferior sector.
• Visual Field:
🞅 OD: MD: −10.5 dB. Upper dense arcuate defect.
🞅 OS: MD: −9.0 dB. Upper nasal step.
Diagnosis: Moderate POAG with borderline control and poor adherence.
Management: Adjuvant SLT to reduce drug burden and achieve target IOP.
• Justification: Based on studies,8,9 SLT in this scenario aims to remove one of the medications or, if these are maintained, reduce IOP to safer levels (additive effect).
• Procedure: SLT 360°.
• Outcome: IOP reduction to 14 mmHg (modest absolute reduction of 4–5 mmHg, common in already medicated eyes). It was possible to discontinue the fixed combination (Timolol/Brimonidine), keeping only the prostaglandin analog at night, which improved adherence.
Case 2: The Polymedicated Patient: Elderly woman, moderate glaucoma, difficulty with adherence and eye drop application.
Case 3
Identification: Female, 65 years old.
Complaint: "My eyes are always red, burning, and feel gritty." Condition worsens when eye drops are applied.
Background: Taking Bimatoprost with preservative (BAK) for two years.
Ophthalmic examination:
• Biomicroscopy: Conjunctival hyperemia 3+/4+, lower diffuse superficial punctate keratitis, reduced break-up time (BUT) (4 s).
• Gonioscopy: Visible open angle, 3/4+ pigmentation.
• Pachymetry: 535 µm.
• IOP: 16 mmHg AO (well controlled, but at the expense of the surface).
• Optic Nerve OCT: Evidence of loss of upper and lower RNFL, with progression analysis showing stability of RNFL and GCC compared to the examinations of the previous two years.
• Visual Field:
🞅 AO: MD: −4.5 dB. Stable for the previous two years.
Diagnosis: Stable POAG + Ocular Surface Disease (OSD) induced/worsened by medication.
Management: Use of eye drops stopped, and SLT used as replacement.
• Justification: The Quality of Life review and the LiGHT data emphasize that the side effects of eye drops are the main cause of reduced quality of life in patients with early glaucoma. SLT eliminates daily exposure to the preservative.
• Procedure: SLT 360°.
• Outcome: After 4 months, IOP was stable at 15 mmHg without medication. There was complete resolution of hyperemia and keratitis, with a drastic improvement in subjective symptom scores.
Case 3: Ocular Surface Disease (Toxicity): Intolerance to preservatives, dry eye, compromised quality of life.
REFERENCES
1. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505-1516.
2. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, and future. Eye (Lond). 2018;32(5):863-876.
3. Kiddee W, Atthavuttisilp S. The effects of selective laser trabeculoplasty and travoprost on circadian intraocular pressure fluctuations: A randomized clinical trial. Medicine (Baltimore). 2017;96(6):e6047.
4. Rubin B, Taglienti A, Rothman RF, et al. The effect of selective laser trabeculoplasty on intraocular pressure in patients with intravitreal steroid-induced elevated intraocular pressure. J Glaucoma. 2008;17(4):287-292.
5. Yuki K, Inoue M, Shiba D, et al. Selective laser trabeculoplasty for elevated intraocular pressure following subtenon injection of triamcinolone acetonide. Clin Ophthalmol. 2010;4:1019-1021.
6. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Six-Year Results of Primary Selective Laser Trabeculoplasty versus Eye Drops for the Treatment of Glaucoma and Ocular Hypertension. Ophthalmology. 2023;130(2):139-151.
7. Freitas AL, Ushida M, Almeida I, et al. Selective laser trabeculoplasty as an initial treatment option for open-angle glaucoma. Arq Bras Oftalmol. 2016;79(6):417-421.
8. Abe RY, Maestrini HA, Guedes GB, et al. Real-world data from selective laser trabeculoplasty in Brazil. Sci Rep. 2022;12(1):1923.
9. Barbosa LEO, Barboza WL, Guedes RP, et al. Selective laser trabeculoplasty as a substitute for medications in patients with mild-to-moderate glaucoma in the Brazilian Public Health System. J Glaucoma. 2024;33(4):303-309.
10. Pillunat KR, Kocket GA, Herber R, et al. Efficacy of selective laser trabeculoplasty on lowering intraocular pressure fluctuations and nocturnal peak intraocular pressure in treated primary open-angle glaucoma patients. Graefes Arch Clin Exp Ophthalmol. 2023;261:1979-1985.
11. Cordeiro FM, Lemos MB, Abe RY, et al. Selective laser trabeculoplasty positively impacts long-term intraocular pressure fluctuation in untreated open-angle glaucoma patients. Lasers Med Sci. 2025;40:363.
12. Garg A, Vickerstaff V, Nathwani N, et al. Efficacy of Repeat Selective Laser Trabeculoplasty in Medication-Naive Open-Angle Glaucoma and Ocular Hypertension during the LIGHT Trial. Ophthalmology. 2020;127(5):590-599.
13. Yang Y, Xu K, Chen Z, et al. Responsiveness to Selective Laser Trabeculoplasty in Open-Angle Glaucoma and Ocular Hypertension. JAMA Ophthalmol. 2024;142(10):918-926.
14. Garg A, Vickerstaff V, Konstantakopoulou E, et al; LiGHT Trial Study Group. Primary Selective Laser Trabeculoplasty for Open-Angle Glaucoma and Ocular Hypertension: Clinical Outcomes, Predictors of Success, and Safety from the Laser in Glaucoma and Ocular Hypertension Trial. Ophthalmology. 2019;126(9):1238-1249.
15. Chavez MP, Guedes GB, Pasqualotto E, et al. Selective Laser Trabeculoplasty Versus Medical Therapy for the Treatment of Open Angle Glaucoma or Ocular Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Glaucoma. 2024;33(12).
16. Kuley B, Zheng CX, Zhang Q, et al. Predictors of Success in Selective Laser Trabeculoplasty. Ophthalmol Glaucoma. 2020; 3(1):9-15.
17. Schlote T, Kynigopoulos M. Selective laser trabeculoplasty (SLT): 1-year results in early and advanced open angle glaucoma. Int Ophthalmol. 2016;36(1):55-61.
18. Prata TS, Guedes GB. SLT: Direto ao Ponto - Manual de Perguntas e Respostas sobre Temas Práticos do Glaucoma. 1.ª ed. Sociedade Brasileira de Glaucoma (SBG); [E-book].
19. Rolim-de-Moura CR, Paranhos Jr A, Loutfi M, Burton D, Wormald R, Evans JR. Laser trabeculoplasty for open-angle glaucoma and ocular hypertension. Cochrane Database Syst Rev. 2022;(8):CD003919.
20. Ojanen ES, Turunen JA, Harju M. The incidence of serious complications after selective laser trabeculoplasty. Acta Ophthalmol. 2025.
21. Wood SD, Elam A, Moroi S. Rare corneal complication following selective laser trabeculoplasty. Am J Ophthalmol Case Rep. 2018;10:28-31.
22. Miranda JF, Maestrini HA, Barbosa CCP, et al. Effect of Anti-Inflammatory Regimen on Selective Laser Trabeculoplasty Outcomes: A Randomized Controlled Trial. J Glaucoma. 2025.
23. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in Glaucoma and Ocular Hypertension (LIGHT) trial. A multicentre, randomised controlled trial: design and methodology. Br J Ophthalmol. 2018;102(5):593-598.
24. Latina MA, de Leon JMS. Selective Laser Trabeculoplasty. Ophthalmol Clin N Am. 2005;18(3):409-419.
| AUTHOR INFORMATION |
|
 |
» Guilherme B. Guedes http://lattes.cnpq.br/6801887455298892 http://orcid.org/0009-0002-9216-0943 |
Funding: The author declare no funding.
Conflicts of interest: The author declares no conflicts of interest.
Received on:
January 14, 2026.
Accepted on:
January 24, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket