

Adriana Ribeiro de Almeida1; Rayssa Medeiros Léda2; Eduardo Damous Feijó3; Augusto Pereira4; André Pena Corrêa Bittencourt5
DOI: 10.17545/eoftalmo/2019.0008
ABSTRACT
PURPOSE. To analyze corneal tomography parameters with Pentacam in patients cared for at Ophthalmology Hospital of Anápolis.
METHODS. Several parameters acquired from Pentacam were analyzed of 180 eyes and differences between the KCN and KCN-suspect groups and the normal group were assessed. This groups were performed using KISA% index.
RESULTS. The study of a group of 180 eyes showed that 81.1% of eyes had no KCN according to the KISA% index, 6.1% had suspected KCN and 12.8% had KCN. There was a significant difference in steep keratometry (K2), maximum axial curvature (Kmax), thinnest corneal location (Pachy Min), thickness at the apex of the cornea (Paqui Apex), Y coordinate of the thinnest corneal location (TLy), asphericity coefficient (QV), progress index maximum (ProgMax) and average (ProgAvg), Ambrosio relational thickness maximum (ARTmax), posterior elevation (PE) in patients with KNC compared to the normal group (p < 0.05). As for the KCN-suspect group, only Kmax, ProgMax and ARTmax were statistically significant compared to the normal group (p < 0.05).
CONCLUSION. The corneal tomography analysis with Pentacam in this study showed a statistically significant difference between the Pentacam parameters in patients with KCN and suspected KCN compared to patients with normal eyes.
Keywords: Cornea; Keratoconus; Corneal Diseases; Diagnostic Imaging; Anterior Eye Segment.
RESUMO
OBJETIVO. Analisar parâmetros de tomografia da córnea com Pentacam em pacientes assistidos no Hospital Oftalmológico de Anápolis.
MÉTODOS. Diversos parâmetros adquiridos a partir do Pentacam foram analisados em 180 olhos, e foram avaliadas as diferenças entre grupos com ceratocone, com suspeita de ceratocone e normal. Estes grupos foram determinados utilizando o índice KISA%.
RESULTADOS. O estudo de um grupo de 180 olhos demonstrou que 81,1% dos olhos não tinham ceratocone de acordo com o índice KISA%, 6,1% tinham suspeita de ceratocone e 12,8% tinham ceratocone. Houve uma diferença significativa em vários parâmetros nos pacientes com ceratocone em relação aos pacientes do grupo normal (p < 0,05): ceratometria no meridiano mais curvo (K2), curvatura axial máxima (Kmax), localização da córnea mais fina (PaquiMin), espessura no ápice da córnea (PaquiApice), coordenada Y do local de menor espessura da córnea (LMEy), coeficiente de asfericidade (QV), índice de progressão máximo (ProgMax) e médio (ProgMed), índice Ambrosio Relational Thinnest máximo (ARTmax) e elevação posterior (EP). Em relação ao grupo com suspeita de ceratocone, apenas a Kmax, ProgMax e ARTmax foram estatisticamente significativas em comparação com o grupo normal (p< 0,05).
CONCLUSÃO. A análise tomográfica da córnea com o Pentacam neste estudo demonstrou uma diferença estatisticamente significativa entre os parâmetros do Pentacam em pacientes com ceratocone e com suspeita de ceratocone em comparação com pacientes com olhos normais.
Palavras-chave: Córnea; Ceratocone; Doenças da Córnea; Diagnóstico por imagem; Segmento Anterior do Olho.
RESUMEN
OBJETIVO. Analizar parámetros de tomografía de la córnea con Pentacam en pacientes que asisten al Hospital Oftalmológico de Anápolis.
MÉTODOS. Diversos parámetros adquiridos desde Pentacam han sido analizados en 180 ojos, y se han evaluado las diferencias entre grupos con queratocono, con sospecha de queratocono y en condición normal. Estos grupos fueron determinados utilizándose el índice KISA%.
RESULTADOS. El estudio de un grupo de 180 ojos ha demostrado que el 81,1% de los ojos no tenían queratocono de acuerdo con el índice KISA%; el 6,1% tenían sospecha de queratocono; y el 12,8% tenían queratocono. Hubo una diferencia significativa en varios parámetros en los pacientes con queratocono respecto a los pacientes del grupo normal (p < 0,05): queratometría en el meridiano más curvo (K2), curvatura axial máxima (Kmax), localización de la córnea más fina (PaquiMin), espesor en el ápice de la córnea (PaquiApice), coordenada Y del lugar de menor espesor de la córnea (LMEy), coeficiente de asfericidad (QV), índice de progresión máximo (ProgMax) y mediano (ProgMed), índice Ambrosio Relational Thinnest máximo (ARTmax) y elevación posterior (EP). Respecto al grupo con sospecha de queratocono, sólo Kmax, ProgMax y ARTmax fueron estadísticamente significativas en comparación con el grupo normal (p< 0,05).
CONCLUSIÓN. El análisis tomográfico de la córnea con Pentacam en este estudio ha demostrado una diferencia estadísticamente significativa entre los parámetros de Pentacam en pacientes con queratocono y con sospecha de queratocono en comparación con pacientes con ojos normales.
Palabras-clave: Córnea; Queratocono; Enfermedades de la Córnea; Diagnóstico por Imagem; Segmento Anterior del Ojo.
INTRODUCTION
Keratoconus (KCN) is a bilateral but typically asymmetric degeneration disorder characterized by progressive protrusion, steepening, and thinning of the corneal stroma1-6. The incidence of KCN has been reported to be approximately 1 per 2000 per year, and the estimated prevalence is 54 per 100,0001-3.
KCN generally manifests as decreased visual quality along with progressive myopia and irregular astigmatism1,4. Corneal thinning generally occurs in the inferior, inferotemporal, or central regions of the cornea4. This ectatic disease has a typical onset at puberty and may progress until after the fourth decade of life, showing progression in 88% of subjects aged up to 19 years3,6.
The etiology of KCN remains unknown, but the literature suggests that it is associated with genetic and environmental factors, such as Down syndrome, allergies, and eye rubbing. Similar forms of ectasia can occur as a complication of refractive surgery in a period of up to 10 years after surgery3,6.
The term suspected KCN is used to define a state of early form of the disease in which the characteristic keratometric or slit lamp findings are absent, but subtle tomographic changes manifest with clinical KCN. Its diagnosis is challenging, and the natural course of the disease cannot be easily predicted because of the frequent presence of corneal manifestations of the disease at the time of diagnosis1,7.
The Pentacam system is a clinical instrument used in ophthalmologic diagnosis that scans the anterior and posterior surface of the cornea with a rotating Scheimpflug camera. The rotating process allows precise measurement of the center of the cornea and also provides pictures in three dimensions1,8.
This study was conducted to analyze the difference between Pentacam parameters in eyes with KCN and suspected KCN compared with normal eyes among patients treated at Ophthalmology Hospital of Anápolis. The findings of this study could be important for defining the presence of corneal ectasia in its earliest stages.
METHODS
This cross-sectional study analyzed the Pentacam data (Oculus Optikgeräte GmbH, Wetzlar, Germany) of 90 patients (180 eyes) who were examined at Ophthalmology Hospital of Anápolis from July 2015 to August 2016. Patients aged 12–80 years were included in this study, whereas those who underwent a previous eye surgery were excluded.
A triage was performed using the KISA% index (Figure 1), in which ≤60% indicates the absence of KCN, between 60% and 100% indicates suspected KCN, and ≥100% indicates KCN.

Several parameters acquired from the Pentacam data were analyzed, and the differences between the KCN and suspected KCN groups and the normal group were assessed using an unpaired Student t-test. All the statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered to be statistically significant.
RESULTS
The 90 study patients included 20 males (22.2%) and 70 females (77.8%) with a mean age of 36.43 years (SD 14.0 years). According to the KISA% index, 81.1% of the eyes had no KCN, whereas 6.1% had suspected KCN and 12.8% had KCN.
The Pentacam parameters of the three study groups are presented in Table 1. A significant difference was observed in steep keratometry (K2), maximum axial curvature (Kmax), thinnest corneal location (Pachy Min), thickness at the apex of the cornea (Paqui Apex), Y coordinate of the thinnest corneal location (TLy), asphericity coefficient (QV), progress index maximum (ProgMax) and average (ProgAvg), Ambrosio relational thickness maximum (ARTmax), and posterior elevation (PE) between patients with KCN and the normal group (P< 0.05). Regarding the suspected KCN group, only Kmax, ProgMax, and ARTmax were statistically significant compared to those in the normal group (P < 0.05) (Table 1).
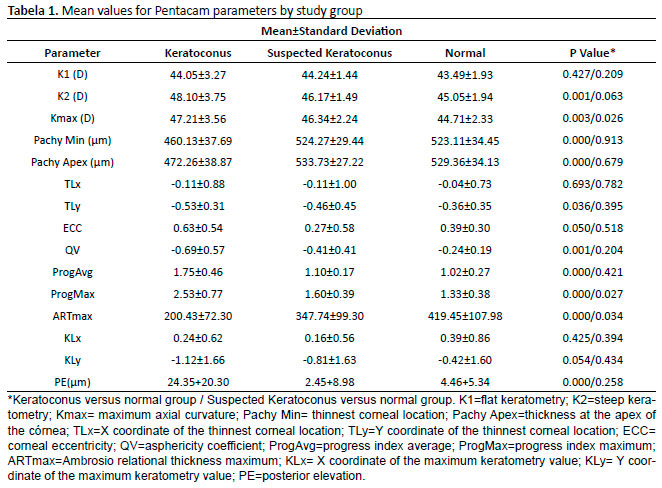
Mean Pachy Min values were 460.13±37.69 µm in KCN eyes, 524.27±29.44 µm in suspected KCN eyes, and 523.11±34.45 µm in normal eyes. The respective mean Pachy Apex values were 472.26±38.87, 533.73± 27.22, and 529.36± 34.13 µm, respectively. Mean PE values were 24.35± 20.30, 2.45± 8.98, and 4.46± 5.34 µm, respectively. Mean flat keratometry (K1) values were 44.05± 3.27, 44.24± 1.44, and 43.49± 1.93 D, respectively. Mean K2 values were 48.10± 3.75, 46.17± 1.49, and 45.05± 1.94 D, respectively. Finally, mean Kmax values were 47.21± 3.56, 46.34± 2.24, and 44.71± 2.33 D, respectively. Other parameters concerning the indexes of pachymetric progression, asphericity, eccentricity, and vertical and horizontal asymmetry were also analyzed (Table 1).
DISCUSSION
KCN generally begins to appear at the age of puberty as a corneal ectatic disorder. It is a progressive condition that can be aggravated in the third decade of life. However, it can be amenable to intervention aimed at preventing a corneal transplant or substantial loss of vision in case this disease is diagnosed early9-11.
Early detection of KCN may help avoid the progression of the condition by corneal cross-linking, thereby preserving the patient’s visual acuity at a relatively good level. Therefore, it is essential to diagnose KCN in an objective, specific, and highly sensitive manner compared with the early forms of the condition, especially in refractive surgery candidates3,12. The literature reports that the prevalence of KCN among refractive surgery candidates is 0.9%–8.1%1.
For diagnosing KCN, ophthalmologists can use complementary tests such as the Pentacam, which is based on the Scheimpflug principle and has software that measures 138,000 elevation points1.The diagnosis of suspected KCN has been a challenge, especially when the ophthalmologic examination does not reveal the suggestive symptoms and clinical signs8,9,13.
Therefore, it is of fundamental importance to use tools such as the Pentacam that aids in an accurate and thorough study of the cornea. Consequently, this examination can provide us an accurate view of the corneal health, and using several parameters, we can infer the presence of KCN even in the initial or suspicious stages9.
This study demonstrated that Pentacam has several parameters that can be used to screen patients with suspected KCN. The knowledge and understanding of each of these parameters is very important for establishing strategies to prevent this primary cause of visual loss1,9.
In our study, we analyzed 15Pentacam parameters between the KCN and normal groups and between the suspected KCN and normal groups. A significant difference was noted in Kmax, ProgMax, and ARTmax between both patients with KCN and those with suspected KCN compared with the normal group (P < 0.05). Based on these data, we can infer that these parameters indicate the presence of the initial development of KCN, alerting the ophthalmologist to a suspected diagnosis of KCN13. The analysis of these parameters is also important to indicate or contraindicate procedures such as refractive surgery to avoid the onset of ectasias1,3,10.
There was also a significant difference in K2, Pachy Min, Pachy Apex, TLy, QV ProgAvg, and PE only in patients with KCN compared with the normal group. However, these parameters showed no statistically significant difference when analyzed between the suspected KCN and the normal groups. These results suggest the importance of these parameters in the evaluation of patients with KCN; however, there was no significant alteration in the suspicion of KCN13.
Studies have shown that the mean values of maximum PE and irregularity were significantly higher in eyes with KCN and suspected KCN than those in control eyes1,11,14. Some of those studies indicate that PE was the most important criterion in the diagnosis of KCN1. Our study demonstrated its statistical significance only for patients with KCN and not for those with suspected KCN compared with normal eyes.
Further research has indicated that the corneal power, thickness, and elevation data exhibited the best predictive accuracy in diagnosing KCN and suspected KCN, with a sensitivity of 97.7% and a specificity of 81.0%1.
Some authors have described lower pachymetry readings in subclinical KCN; however, they did not find statistically significant differences in this parameter between suspected KCN eyes and normal eyes1,14,15, which corroborates our findings.
The present study also demonstrated no statistically significant differences in K1, ECC, TLx, KLx, and KLy between all the comparative groups. Our findings are consistent with similar results reported in the literature13.
The corneal tomography analysis using Pentacam in this study revealed a statistically significant difference between the tomographic indexes in patients with KCN and those with suspected KCN compared with patients with normal eyes. Identifying the suspected KCN cases is important to establish adequate follow-up for early intervention in case the disease manifests itself or to be cautious in indicating procedures such as refractive surgery that may predispose to the occurrence of corneal ectasias.
CEP APPROVAL
Committee on Ethical Research of the Ophthalmologic Hospital of Anapolis (protocol #032/2018)
REFERENCES
1. Serdarogullari H, Tetikoglu M, Karahan H, Altin F, Elcioglu M. Prevalence of keratoconus and subclinical keratoconus in subjects with astigmatism using pentacam derived parameters. J Ophthalmic Vis Res. 2013; 8(3):213-219.
2. Steinberg J, Aubke-Schultz S, Frings A, Hülle J, Druchkiv V, Richard G, et al. Correlation of the KISA% index and Scheimpflug tomography in ‘normal’, ‘subclinical’, ‘keratoconus-suspect’ and ‘clinically manifest’ keratoconus eyes. Acta Ophthalmol. 2015 May; 93(3):199-207.
3. Ruiz Hidalgo I, Rozema JJ, Saad A, Gatinel D, Rodriguez P, Zakaria N, et al. Validation of an objective keratoconus detection system implemented in a scheimpflug tomographer and comparison with other methods. Cornea. 2017; 36(6):689-695.
4. Ucar M, Cakmak HB, Sen B. A statistical approach to classification of keratoconus. Int J Ophalmol. 2016; 9(9):18.
5. Li X, Yang H, Rabinowitz YS. Keratoconus: classification scheme based on videokeratography and clinical signs. J Cataract Refract Surg. 2009; 35(9):1597-1603.
6. Ameerh MAB, Bussières N, Hamad GI, Bdour MDA. Topographic characteristics of keratoconus among a sample of Jordanian patients. Int J Ophthalmol. 2014; 7(3):714-719.
7. Rabinowitz YS, Rasheed K. KISA% index: a quantitative videokeratography algorithm embodying minimal topographic criteria for diagnosing keratoconus. J Cataract & Refractive Surg. 1999; 25(10):1327-1335.
8. Jain R. Pentacam: principle and clinical applications. J Curr Glaucoma Prac. 2009; 3(2):20-32.
9. Hashemi H, Beiranvand A, Yekta A, Maleki A, Yazdani N, Khabazkhoob M. Pentacam top indices for diagnosing subclinical and definite keratoconus. J Curr Ophthalmol 2016; 28:21-26.
10. Li Y, Meisler DM, Tang M, Lu AT, Thakrar V, Reiser BJ, et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology. 2008; 115(12):2159-2166.
11. Gomes JAP, Tan D, Rapuano CJ, Belin MW, Ambrósio Jr R, Guell JL, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015; 34:359-369.
12. Sadoughi MM, Feizi S, Delfazayebaher S, Baradaran-Rafii A, Einollahi B Shahabi C. Corneal changes after collagen crossslinking for keratoconus usin dual scheimpflug imaging. J Ophthalmic Vis Res. 2015; 10(4):358-363.
13. Hashemi H, Beiranvand A, Yekta A, Maleki A, Yazdani N, Khabazkhoob M. Pentacam top indices for diagnosing subclinical and definite keratoconus. J Curr Ophthalmol. 2016; 28(1):21-26.
14. Martínez-Abad A, Piñero DP, Ruiz-Fortes P, Artola A. Evaluation of the diagnostic ability of vector parameters characterizing the corneal astigmatism and regularity in clinical and subclinical keratoconus. Cont Lens Anterior Eye. 2017; 40(2):88-96.
15. Bao F, Geraghty B, Wang Q, Elsheikh A. Consideration of corneal biomechanics in the diagnosis and management of keratoconus: is it important? Londres: Eye Vis. 2016; 3:18.





Funding: No specific financial support was available for this study
Disclosure of potential conflicts of interest: The authors have no potential conflicts of interest to disclose
Received on:
October 22, 2018.
Accepted on:
February 7, 2019.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket