

Sidney Julio Faria e Sousa1; Milton Ruiz Alves2
DOI: 10.17545/eoftalmo/2018.0004
ABSTRACT
Astigmatism designates either an optical aberration or an ametropia. Although the astigmatic aberration is a fundamental part of the astigmatic ametropia, these two entities are conceptually different. The former is independent of the eye, and the latter closely relates to it. This article explores the differences between the aberration and ametropia, by exploiting the particularities of each concept.
Keywords: Astigmatism; Refractometry; Refractive Errors.
RESUMO
Astigmatismo refere-se a uma aberração óptica ou a uma ametropia. Embora a aberração astigmática seja parte fundamental da ametropia astigmática, as duas entidades são conceitualmente diferentes. A primeira independe do olho, enquanto que a segunda está intimamente relacionada a ele. Este artigo analisa as diferenças entre aberração e ametropia, explorando as particularidades de cada conceito.
Palavras-chave: Astigmatismo; Refratometria; Erros de Refração.
RESUMEN
Astigmatismo es el nombre que se da a una aberración óptica o una ametropía. Aunque la aberración astigmática sea parte fundamental de la ametropía astigmática, las dos entidades son distintas en su concepto. La primera es independiente del ojo, y la última se relaciona íntimamente con él. Este artículo explora las distinciones entre la aberración y la ametropía, presentando las particularidades de cada concepto.
Palabras-clave: Astigmatismo; Refractometría; Errores de Refracción.
INTRODUCTION
Astigmatism designates either an optical aberration or an ametropia. Although astigmatic aberration is a fundamental part of astigmatic ametropia, these two entities are conceptually different. The former is independent of the eye, and the latter closely relates to it. This article explores the differences between aberration and ametropia, by exploiting the particularities of each concept. Astigmatism can be regular or irregular. We will address only the former type.
ASTIGMATISM AS AN OPTICAL ABERRATION
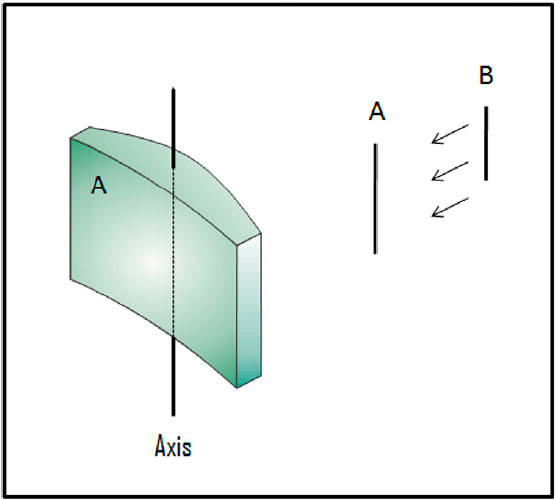
Astigmatism is an optical aberration associated with the toric refractive surfaces found in toric lenses. A toric surface is a technical name for the surface of a doughnut, which has two spherical curves with different radii that cross perpendicularly. The principal meridians of toric lenses are those that contain these curves.
For each object point, the toric refractive surface generates two image lines placed separately at right angles on the sagittal line that crosses its optical center. If the object point is at infinity, each image line becomes a focal line1. The very formation of a proximal and a distal focal line for each object point configures an optical aberration, namely, astigmatic aberration or astigmatism. It is an aberration because one would expect a single focal point for each object point. The gap between the two focal lines is known as Sturm’s interval. Its size, in diopters, measures the amount of astigmatism (Figure 1).
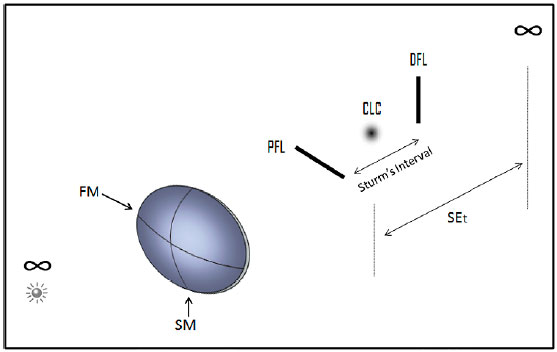
Each focal line derives from the principal meridian that is perpendicular to it: the proximal focal line comes from the steepest meridian and the distal focal line from the flattest one. In the dioptric center of the Sturm’s interval sits a circular blur called the circle of least confusion (CLC). Despite the plethora of blurs in and out of this interval, the CLC is the only one of interest, and the only one displaying a circular shape. (Figure 1).
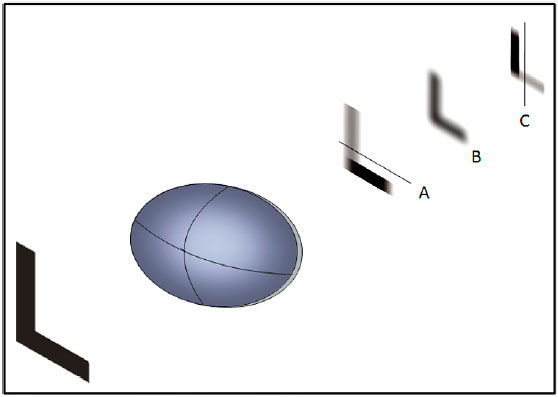
At the level of each focal plane, the image derived by refraction from a single object point concentrates in a distinct focal line with a specific direction. The collection of all focal lines derived from the whole set of points of the object of fixation forms an extended image with a definite directional blurring. In areas where the inclination of the blur matches the direction of the details of the scene, the density of the background enhances; in places where this condition is unfulfilled, the background fades in proportion to the degree of the directional mismatching between these variables. The irregular combination of patches of contrast augmentation and fading cause a type of image degradation called confusion. Figure 2 (A and C) shows the letter L at both the proximal and distal focal planes. Note that the image confusion relates to the direction of the focal lines. Image degradation is proportional to both the amount of astigmatism and degree of mismatching between the background texture and focal line orientation. At the CLC plane, the directional blurring disappears; things are still fuzzy but not confusing, as shown in Figure 2(B). The homogeneous spreading of the points in this site (there are no lines here) explains its lack of directional blurring; this is where the astigmatic system is best at reproducing the profile of the light source.
Whenever the average power of a toric lens is of interest, the CLC is the reference for its measurement. The average power or spherical equivalent of a toric lens (SEt) is the dioptric distance of its CLC from infinity (Figure 1). For instance, if the CLC is at infinity SEt is null. If it is +3D from infinity (0.33 meters from a converging toric lens), SEt = +3 D. The SEt of diverging surfaces carry negative signs.
Toric lenses with SEt = 0 are called cross cylinders. They represent the combination of two cylindrical lenses of the same power, opposite signs, and axes at right angles. For example, the association +1 cyl 90º x -1 cyl 180º is a cross cylinder. On the other hand, cylindrical lenses (or cylinders) are particular forms of toric lenses where one of the principal meridians has zero power. They produce only a single focal line that is always parallel to their axes of revolution. The name comes from their resemblance to cylindrical pieces of refractive material.
One may express a cross cylinder as either a combination of two cylinders or an association of a spherical and a cylindrical lens. In its spherocylindrical form, the sphere always has half of the power of the cylinder with the opposite sign. Thus, once given a cylinder -2cyl 180º one has just to combine it with a sphere of +1 D to create a cross cylinder of +1 sph x −2 cyl 180. In practical terms, this combination is identical to + 1 cyl 90 x -1 cyl 180. Cross cylinders have great importance in both the diagnosis and correction of astigmatic refractive errors.
Whenever the direction of the incident light forms an angle with the optical axis of a spherical lens, the resulting image (radial or off-axis astigmatism) has the same features of the aberration generated by toric lenses. While having some significance in clinical practice, the chief importance of this type of astigmatism is in the field of instrumental optics2.
ASTIGMATISM AS AN AMETROPIA
Ametropia is a failure of the unaccommodated eye to focus on the retina light rays coming from infinity. In spherical ametropias like hyperopia and myopia, the problem comes from a mismatch between the power of the eye system and its axial length, leading to an unfocused image on the retina. To neutralize an ametropia means to find a lens that focuses the image on the retina. In hyperopia, where the relative power an eye is too weak for its size, it requires a spherical converging lens; in myopia, where an eye is too strong for its size, it needs a spherical diverging lens.
Many human eyes have corneas that behave like convex toric lenses, generating for each object point at infinity three images of clinical interest: a proximal focal line, a CLC, and a distal focal line. These features configure a particular kind of ametropia called astigmatic ametropia or astigmatism (Figure 3). The way the astigmatic eye sees depends mostly on which of the three images is closest to the retina.
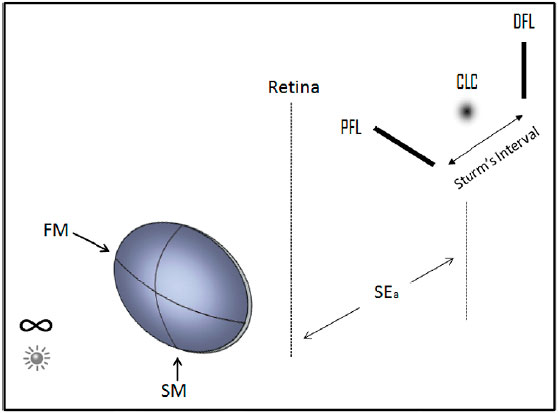
At this point, the following question is pertinent: What is the difference between astigmatic aberration and astigmatic ametropia? The answer is the presence of the eye. The existence of the eye is irrelevant for the understanding of the aberration but critical for the comprehension of the ametropia. Although both concepts have features in common ─ two image lines and a CLC ─ the retina is the element that distinguishes the refractive error. Astigmatic ametropia combines an astigmatic aberration, evidenced by the extent of the Sturm’s interval, with a spherical error, quantified by the displacement of the CLC from the retina (Figure 3). Astigmatic ametropias are classified as myopic, hyperopic, or mixed according to the position of the boundaries of Sturm’s interval relative to the retina3. It is myopic when both focal lines are in front of the retina, or one of them is in front of, and the other is on the retina. It is hyperopic when both focal lines are behind the retina, or one of them is behind, and the other is on the retina. If Sturm’s interval straddles the retina, the astigmatism is mixed. Mixed astigmatism is an ambiguous concept that recognizes a CLC in front, behind, and on the retina. It gathers though different scenarios under a single name. This problem stems from the use of Sturm’s interval instead of the CLC as a reference.
The spherical power that puts the CLC on the fovea is the spherical equivalent of astigmatic ametropia (SEa). It is the spherical component of the astigmatic ametropia (Figures 3 and 4B). The dependence of this parameter on the position of the CLC emphasizes the significance of the latter in the characterization of astigmatic ametropia. One should distinguish the spherical equivalent of a toric lens from the spherical equivalent of an astigmatic ametropia. The former represents the average power of a toric lens, defined by the dioptric distance of the CLC from infinity. The latter applies to astigmatic ametropias and specifies the power needed to put the CLC on the retina. Compare SEt with SEa in Figures 1 and 3.
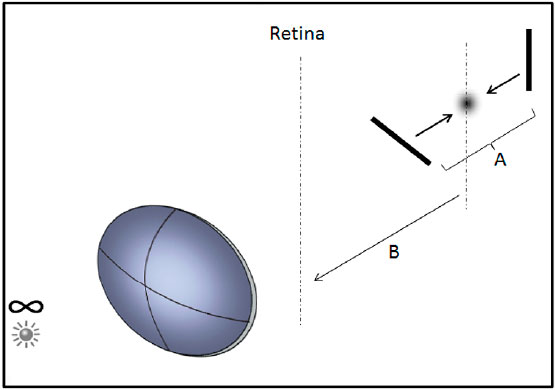
Neutralizing an astigmatic aberration means collapsing Sturm’s interval. As it contracts, the lengths of the focal lines and the size of the CLC shrink progressively to merge into a single point. The collapsing of Sturm’s interval demands cylindrical lenses since spherical lenses only change the position of the whole interval relative to the retina. Cylindrical lenses reduce Sturm’s interval in three ways: by pulling the distal focal line toward the proximal, by pushing the proximal focal line toward the distal, or by doing both actions simultaneously (Figure 4A). To maximize the effect of these actions, one has to align the axis of the corrective cylinder with the focal line in motion (Figure 5). Thus, to pull the distal focal line (toward the proximal) one needs a converging cylindrical lens with an axis in perfect alignment with it. To push the proximal focal line (toward the distal) one needs a diverging cylindrical lens with an axis in perfect alignment with it. Finally, to undo Sturm’s interval, acting on both focal lines, one has to use a cross cylinder with the axis of the converging cylinder aligned with the distal focal line, and the axis of the diverging cylinder aligned with the proximal focal line.
Regarding the correction of astigmatic aberration, these three procedures are equivalent. On the other hand, they have distinct effects on the spherical power of astigmatic ametropia. Converging cylinders collapse Sturm’s interval by placing the images closer to the cornea. Diverging cylinders do the same by setting the images further from the cornea. Cross cylinders do not disturb the position of the image at the CLC. In other words, converging cylinders tend to decrease, diverging cylinders to increase, and cross-cylinders to preserve the accommodative effort of the eye.
Once fully corrected the astigmatic aberration, all that remains is an image point. If it is in the vitreous body, one can move it to the fovea with a diverging lens. If it is behind the eye, the procedure requires a converging spherical lens. The final correction of an astigmatic ametropia usually winds up in a spherocylindrical combination. For instance, +4 sph x -2 cyl 30º expresses the combination of a spherical lens of +4 D with a cylinder of −2 cyl 30º. However, one should be aware that the spherical power of this combination is not the one suggested by the refractive expression (+4 D), but the spherical equivalent of the resulting spherocylinder (+3 D).
In conclusion, astigmatism is an ambiguous term because it identifies either an optical aberration or a refractive error. Its current classification is also inadequate because it leads to ambiguities when Sturm’s interval straddles the retina. One could devise a better classification system using the spherical equivalent as a reference point, considering its critical importance in many fields of ophthalmic optics, namely, refractive surgeries, intraocular lens implantation, contact lenses, and prescription of eyeglasses. A distinctive name for astigmatic ametropia would be another improvement. An option for it already exists in the literature4,5. Our preference is for astigmopia.
REFERENCES
1. Faria-e-Sousa SJ, Victor G, Ruiz Alves M. Visual optics under the wavefront perspective. Arq Bras Oftalmol. 2014; 77(4), 267-270. https://doi.org/10.5935/0004-2749.20140068
2. Rubin M. Radial Astigmatism In:Optics for Clinicians. 2nd ed, Gainsville, FL:TRIAD Scientific;1977. p. 286-289
3. Duke-Elder S, Abrams D. The optical condition in astigmatism. In: Duke-Elder S, editor. Ophthalmic Optics and Refraction, System of Ophthamology, Vol. V. London: Henry Kimpton; 1970. p. 283 - 284.
4. Tour RL. Astigmatism. In: Gettes BC, editor. Refraction. London: J & A Churchill Ltd; 1965. p. 27-47.
5. Astigmia. [Internet]. Available from: www.merriam-webster.com/medical/astigmia

Funding: No financial support was available for this study.
CEP Approval: Not applicable.
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
February 5, 2018.
Accepted on:
March 15, 2018.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket