

Sidney Julio Faria e Sousa1; Stella Barretto2
DOI: 10.17545/eOftalmo/2017.100
ABSTRACT
The first successful corneal transplantation used tissue from a living donor. The preservation of corneas gained momentum only after Filatov showed that a cadaver´s eye, when stored at low temperature, could be a source of viable corneas for transplants. Three methods proved to be useful for this purpose: moist chamber, cryopreservation, and liquid medium storage. They were introduced in that order. The first provides cold storage of corneas in situ for up to 2 days after death. It is still useful in underdeveloped regions of our planet. Eye banks practically abandoned the second method due to its complexity. Currently, the most popular storage technique is the third. Depending on the composition of the liquid medium, it allows for cold or warm preservation of the cornea ex situ. This article describes the characteristics of the three storage systems in quasi-chronological sequence.
Keywords: Corneal transplantation; Eye banks; Tissue preservation.
RESUMO
O primeiro transplante de córnea bem sucedido utilizou tecido de um doador vivo. A preservação das córneas somente ganhou impulso após Filatov ter demonstrado que o olho de cadáver, quando armazenado a baixa temperatura, poderia ser uma fonte de córneas viáveis para transplantes. Três métodos revelaram-se úteis para este fim: câmera úmida, criopreservação e armazenamento em meio líquido Estes métodos emergiram nesta ordem apresentada. O primeiro, fornece armazenamento frio de córneas in situ por até dois dias após a morte, sendo este método ainda útil nas regiões pobres do nosso planeta. Os bancos de olhos praticamente abandonaram o segundo método devido à sua complexidade. Atualmente, a técnica de armazenamento mais popular é a terceira. Dependendo da composição do meio líquido, é possível preservar a córnea a frio ou à temperatura ambiente ex situ. Este artigo descreve as características dos três sistemas de armazenamento em uma sequência quase cronológica.
Palavras-chave: Transplante de córnea; Bancos de olhos; Preservação de tecido.
INTRODUÇÃO
The clash of French and English troops in Egypt between 1798 and 1801 as part of the Napoleonic Wars caused the contact of a significant number of European soldiers with Trachoma. 1 The return of the fighters to the origin generated Trachoma epidemics in London, Paris, and Brussels, in 1801, 1806, and 1815, respectively.2 Corneal transplantation arose from the intention to treat corneal opacity resulting from these epidemics. In 1824, Franz Reisinger 3 presented the penetrating corneal transplant, which he called keratoplasty. The proposal was derived from an experimental study in rabbits. He did not perform surgery on humans, but suggested that corneas could be sourced from animals. Countless unsuccessful attempts at performing both penetrating and lamellar corneal transplantation characterized the efforts in this field in the nineteenth century. During this period, the primary source of grafting was the eyes of animals, due to the ease of availability and ignorance about immunological intolerance. 4 Powers, in 1873, was the first to recommend the use of allografts instead of xenografts, due to the similarity in texture and thickness between the donor and recipient corneas 5. In 1905, Zirm 6 performed the first successful transplant in humans, with a cornea harvested from a living donor. The fact overturned Fuchs's theory that generalized graft opacity was an inherent part of the healing process of the transplanted cornea. 7 From this date onwards, surgeons started using tissue from living donors, whose eyes had suffered severe trauma without corneal involvement. One possible motivation for excision of these eyes was the fear of sympathetic uveitis.
Cold preservation of the cornea in situ
In 1935, Filatov 8 published his observation that eyes kept at 4°C in hermetically sealed glass vials could keep the cornea viable for transplants for up to 56 h after death. This observation contained two revolutionary concepts: that the corneas could temporarily survive the death of the donor and that hypothermia could extend the cells’ period of vitality. Assuming that the eyeballs might be contaminated, he also advised bathing them with bright green solution at 1:2000. Over time, these vials gained a lining of gauze or cotton wool soaked in saline solution, instituting a moist chamber when sealed. In this housing, the cornea is stored in situ at 4°C. At the time of surgery, it is excised from the eye by trepanation through the epithelial side. This method of storage gave birth to the eye bank stricto sensu, represented by a refrigerator that stores eyes in moist chambers. In 1944, Paton and Aida Breckinridge 9 created the eye bank lato sensu– an institution for the harvesting, storing, analysis, and distributing corneas for transplantation. As experience with corneal grafting improved, it became clear that that the safe interval of preservation in the moist chamber was up to 48 h after death. This time constraint started to be challenged in 1954 when Stoker 10 convincingly demonstrated that the endothelium is responsible for the maintenance of corneal transparency by actively exchanging electrolytes between the stroma and the anterior chamber. This fact had a decisive role in the perception that the endothelium was the primary object of concern in the endeavor to extend the period of post-mortem corneal vitality.
In 1968, Mizukawa and Manabe 11,12 described a liquid medium for corneal storage in situ at 4°C containing tissue culture solution 199, chondroitin sulfate, ATP precursors, penicillin, and streptomycin. By exchanging the medium on alternate days, the corneal preservation could be made effective for up to 4 days. Although this method had little repercussion outside Japan, it has taken its place in history as the first liquid medium to preserve the cornea at low temperature using a cell culture medium enriched with chondroitin sulfate, cell metabolism stimulants, and antibiotics.
Cold preservation of the cornea ex situ
In 1974, McCarey-Kaufman (M-K) presented a liquid storage medium to be kept at 4°C, capable of maintaining endothelial vitality for up to 4 days. 13,14 Unlike the Japanese method, the cornea was preserved outside the eyeball bounded by a scleral rim. The advantage of this system was simplicity and low cost. The storage solutions were marketed in transparent vials, allowing for endothelial inspection in the slit lamp and cell counting under specular microscopy (see Figure 1). The original formulation consisted of a mixture of tissue culture 199, bicarbonate buffer, dextran, and antibiotics. Subsequently, HEPES and phenol red indicator replaced bicarbonate buffer to stabilize and monitor the pH. 15

Although the M-K medium extended the preservation time for only 2 days relative to the moist chamber, it granted enough flexibility to convert keratoplasty to an elective procedure. With this improvement, corneal transplants gained significant momentum. The trepanation of the graft from the endothelial side also gained popularity, stimulating ingenious modifications in cutting instruments for the cornea. Surgeons had been acquainted with corneoscleral buttons since 1965, in association with cryopreservation of the cornea 16. However, only a restricted group of them had access to this laborious method of corneal storage.
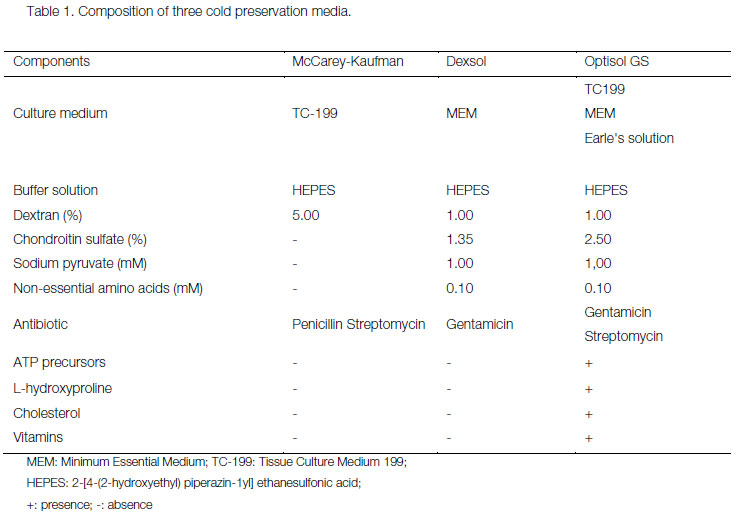
As a whole, liquid storage media for cold preservation contain the following components: (1) cell culture solution; (2) buffer solution; (3) hyperosmotic agent; (4) pH indicator; (5) antibiotics, and additives (6).
Cell culture solutions are balanced salt solutions with cellular nutrients, amino acids, vitamins, carbohydrates, and cofactors. They maintain the vitality of cells, tissues, and organs in an artificial environment. 17 The most frequently used are TC-199, MEM, or the combination of both with Earle's solution. Buffers are aqueous solutions of weak acids with their conjugate bases that maintain the pH around 7.4. Bicarbonate buffer and HEPES are the most popular in the eye-bank field. Hyperosmotic agents reduce the corneal edema associated with liquid medium preservation. 12 This phenomenon is a direct consequence of the generalized post-mortem depression of the metabolic activity of corneal cells, particularly those of the endothelial layer. The hyperosmotic agents used in cold preservation are dextran and chondroitin sulfate. The former is more efficient than the latter, despite being more toxic to the endothelium, particularly at concentrations equal to or greater than 5%. 12 Chondroitin sulfate has the additional effect of protecting the endothelial cells, when used at low temperature and in the right concentration. 12,18 Modern storage media use combinations of both agents in concentrations lower than those of individual agents traditionally used to promote satisfactory and safe dehydration of the endothelium. 19 The prevailing pH indicator is phenol red, which gives the medium a pinkish coloration at pH 7.4. Above this value, it becomes red; below it, it turns yellow. The yellow color suggests microbial contamination of the medium. Antibiotics are the final defense against colonization of the corneoscleral button. The first combination of antibiotics employed was penicillin with streptomycin. 11,13 Current media use gentamicin with streptomycin. 19 The usual dose of these antibiotics is in the range of 80–100 µg/ml. Additives are substances introduced into the liquid medium to counterbalance the deleterious effects of cold temperature and preservation time on the endothelium. They include antioxidants, such as glutathione; collagen stabilizers, such as L-hydroxyproline; ATP precursors, such as adenine, adenosine, and inosine; sources of energy, such as sodium pyruvate; vitamins such as ascorbic acid, calciferol, niacin; and micronutrients. 19 The formulation of these elements is generally protected by industry confidentiality.
In 1984, Kaufman and associates 20 introduced K-Sol medium (Cilco, Huntington, West Virginia), whose novelty was the substitution of 5% dextran by 2.5% chondroitin sulfate. The latter agent was critical for extending the period of tissue preservation to 1 week, despite an initial expectation of twice as long. The problem with this replacement was that chondroitin sulfate alone did not have enough osmotic power to prevent preservation-induced corneal edema. 12 In an attempt to solve this impasse, various combinations of the main constituents of the storage media were tested, giving rise to new commercial formulations. Among these, Dexsol and Optisol GS (Chiron Ophthalmics, Irvine, California) stand out for their widespread use. Both preserve corneas for up to 14 days at 4°C, although the latter is superior regarding the preservation of cellular morphology as well as in maintaining the original thickness of the cornea. 19,21 The basic formulations of the M-K, Dexsol, and Optisol GS media are shown in Table 1. The most recent intermediate-term medium for corneal preservation at 4°C, approved by the FDA in 2007, is Life4C (Numedis Inc, Isanti, Minnesota). Although it contains supplements such as recombinant human insulin, glutathione, and others, its performance seems to be similar to that of Optisol GS. 22
Warm preservation of the cornea ex situ
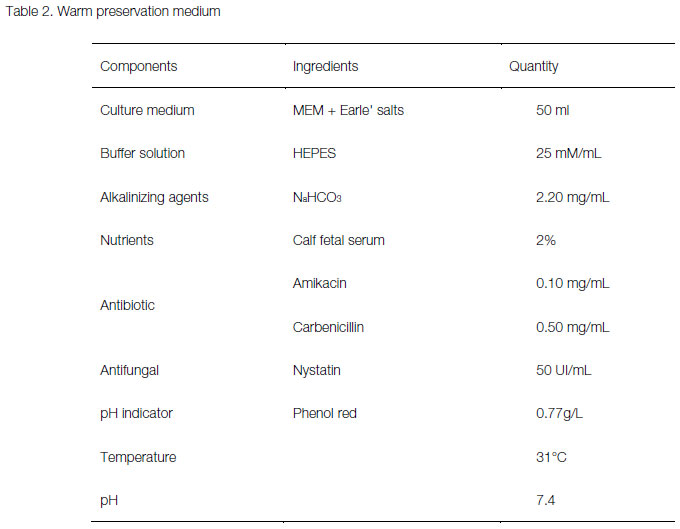
Warm preservation of the cornea is best known as organ culture storage. Doughman implemented the method in 1976. 23 In this procedure, the corneoscleral button is stored in a liquid medium for 4 weeks at temperatures varying from 31°C to 37°C, according to the method of preference. 24 Another difference among methods is in the renewal of the solution during the storage period. Some eye banks do not change it, and others renew it every 1 or 2 weeks. 25,26
At warm temperatures, endothelial cells tend to ingest the hyperosmotic agents, which eventually become toxic to them. 27 Consequently, these agents are not used on a regular basis in organ culture preservation. The problem with their absence is that the preserved corneas acquire twice their normal thickness. To counterbalance this event and return the corneas to their original thickness and transparency, it is necessary to dip the corneoscleral button into a transport medium supplemented with dextran at concentrations varying from 4% to 8%, immediately before sending it to the surgeon. 25,28 The maximum period of tissue immersion ranges from less than 1 day to 7 days, at the discretion of the eye bank. 28 Tissue swelling associated with the organ storage medium does not allow for slit lamp analysis nor specular microscopy of the endothelium. Identification of the endothelial cells requires dilation of the intercellular spaces, which is done by plunging the cornea into a 0.4% solution of NaCl and observing the endothelial mosaic under optical microscopy with long-range objectives. 29 The interpretation of the findings requires extensive experience, as the endothelium configuration varies with the composition of the medium and the period of storage. 30To test sterility, one sample is cultured on the seventh day of preservation and another immediately before releasing the cornea for transplantation.31
The main advantage of warm over cold preservation is the length of tissue preservation, which is twice that of the best cold preservation medium. The extended period of storage not only increases the time for tissue analysis but also attenuates the fluctuation of corneal accessibility. Other alleged advantages of this system include better monitoring of medium sterility, as contamination becomes rapidly evident in warm temperatures; 28 the retention of the in vitro healing capability of the endothelial layer through cell hypertrophy and sliding; 32 and the possibility of invigorating the corneal endothelium by transferring the cornea from an expiring hypothermic medium to organ culture storage. 33 Nonetheless, the practical importance of these attributes to graft survival still needs a convincing demonstration. On the downside, organ culture preservation is more time and labor intensive than cold storage. The obligation to check the sterility of the medium, the invasive technique for endothelial analysis, and the dependence on a transport medium prevent the immediate use of the cornea. The overall cost of the method tends to be higher because of the need to maintain a more sophisticated laboratory with highly specialized personnel. Although the composition of organ culture media varies with the preferences of each eye bank, most of them contain the same essential ingredients. Table 2 shows an example of a formulation for comparison with that of cold preservation media. 29
Cryopreservation
In 1965, Chapel-Kaufman-Robins 16 launched the first practical and reliable method of cryopreservation of the cornea. This process requires the dipping of the corneoscleral button for 10 min in four 1-ml solutions of human serum albumin, with increasing concentrations of dimethyl sulfoxide and sucrose. The vial containing the last bath is sealed and refrigerated in a controlled manner to −80°C and then transferred to a liquid nitrogen tank at −160°C. At the time of surgery, a staff member reheats the vial in water at 56°C until an ice ball forms in the center of the tissue. Next, the cornea is withdrawn from the vial and placed in 1 ml of human albumin solution at 4°C for at least 10 min and held at that temperature until the moment of its use.
The advantage of cryopreservation is in keeping the tissue alive indefinitely. The downside is that the process is laborious, requiring sophisticated logistics and highly skilled personnel. Donors must be under 50 years of age, and the corneas must be preserved within a few hours of death. 34,35 Because of these limitations, the method did not become popular. However, some eye banks, such as the Indianapolis Lions Eye Bank, used it successfully until the late 1980s when medium-term storage media gained widespread use.
FINAL CONSIDERATIONS
Presently, the dominant system of corneal preservation is ex situ corneal storage in a liquid medium at a cold or warm temperature. Each of these two modalities offers several options. Three issues are relevant to the choice of a medium: local availability, cost, and storage period. The last feature is the most challenging, given the difficulty of verifying the information advertised by the manufacturers. Part of the problem is the absence of an objective method for checking endothelial function. The maximum preservation time, for example, is not directly inferred from the activity of the endothelial layer, but from its morphological and histochemical characteristics in vitro, as well as from the fate of the grafts in the long run. This kind of information is far from ideal, being influenced by a multitude of factors like donor age, time and cause of death, etc. Accordingly, all methods of corneal storage have shown, with time, a shorter period of protection than initially expected. Because of this, the European Eye Bank Association suggests anticipating the use of the cold-preserved tissue well before the maximum preservation time provided by the manufacturer. In the case of Optisol, it should be between 7 and 10 days of storage. 28 Nevertheless, the validity of this precaution still needs confirmation.
REFERENCES
1. Meyerhof M. A short history of Ophthalmia during the Egyptian campaigns of 1798-1807. Br J Ophthalmol. 1932;16(3):129-152. https://doi.org/10.1136/bjo.16.3.129
2. Schlosser K. History of trachoma. Disponível em: https://www.nps.gov/elis/learn/education/upload/Trachoma-Through-History-2.pdf
3. Reisinger F. Die keratoplastik ein Versuch zur Erweiterung der Augenheilkunst. Bayerische Annalen.1824;1:207-215
4. Paton RT. History of corneal grafting. In: Keratoplasty. New York: McGraw-Hill Book Co., Inc. 1955, p.10
5. Power H: On transplantation of the cornea. Fourth International Congress Ophthalmol. London, 1872;4:172-176
6. Armitage WJ, Tullo AB, Larkin DFP. The first successful full-thickness corneal transplant: a commentary on Eduard Zirm's landmark paper of 1906. Br J Ophthalmol. 2006 Oct; 90(10): 1222–1223. https://doi.org/10.1136/bjo.2006.101527
7. Fuchs E: Ueber Keratoplastik. Wien Klin Wochenschrift 1894;7:843-845
8. Filatov VP. Transplantation of the cornea. Arch Ophthamol.1935;13(3):321-347. https://doi.org/10.1001/archopht.1935.00840030011001
9. The eye-bank for sight restoration, Inc. : Mission&History http://www.eyedonation.org/mission-and-history.html
10. Stocker FW. The endothelium of the cornea and its clinical implications. Trans Am Ophthalmol Soc. 1953; 51;669-786. PMid:13216798 PMCid:PMC1312580
11. Mizukava T, Manabe R. Recent advances in keratoplasty with special reference to the advantage of liquid preservation. Nihon Ganga Kiyo 1968; 19 (12):1310-1318
12. Lindstrom RL. Advances in corneal preservation. Tr Am Ophthalmol Soc 1990;88:555-648. PMid:1710084 PMCid:PMC1298601
13. McCarey BE, Kaufman HE. Improved corneal storage. Invest Ophthalmol Vis Sci. 1974; 13(3):165-173. https://doi.org/10.1016/0002-9394(75)90273-1
14. Aquavella JV, Van Horn DL, Haggerty CJ. Corneal preservation using M-K medium. Am J Opththalmol. 1975; 80(5):791-799. https://doi.org/10.1016/0002-9394(75)90273-1
15. Waltman SR, Palmberg PF. Human penetrating keratoplasty using modified M-K medium. Ophthalmic Surg 1978;9(2);48-50. https://doi.org/10.1001/archopht.1965.00970040671015
16. Capella JA, Kaufman HE, Robbins JE. Preservation of viable corneal tissue. Arch Ophthalmol. 1965; 74(5):669-673. https://doi.org/10.1001/archopht.1965.00970040671015
17. Arora M. Cell culture media: A review. Labone (The world of laboratories) https://doi.org/10.13070/mm.en.3.175
18. Yau C, Kaufman HE. A medium-term cornel preserving medium (K-Sol). Arch Ophthalmol 1986; 104(4);598-601. https://doi.org/10.1001/archopht.1986.01050160154032
19. Lindstrom RL, Kaufman HE, Skelnik DL, Laing RA et al. Optisol corneal storage medium. Am J Ophthalmol. 1992;114(3):345-356. https://doi.org/10.1016/S0002-9394(14)71803-3
20. Kaufman HE, Varnell ED, Kaufman S. Chondroitin sulfate in a new cornea preservation medium. Am J Ophthalmol. 1984; 98(1):112-14. https://doi.org/10.1016/0002-9394(84)90198-3
21. Kaufman HE, Beuerman RW, Steinemann TL, Thompson HW, Varnell ED. Optisol storage medium. Arch Ophthalmol. 1991;109(6):864-868. https://doi.org/10.1001/archopht.1991.01080060128040
22. Pham C, Erik Hellier E, Vo M et al. Endothelial specular image quality in Optisol GS and Life4˚C. Int J Eye Banking2013;1(2): 1-8. https://doi.org/10.7706/ijeb.v1i2.52
23. Doughman DJ, Harris JE, Schmitt KM. Penetrating keratoplasty using 37° C organ cultured cornea. Trans Am Acad Ophthalmol Otolaryngol. 1976;88:778–793. https://doi.org/10.1007/BF00154722
24. Pels E, Schuchard Y. Organ-culture preservation of human corneas. Doc Ophthalmol. 1983;56:147–153. https://doi.org/10.1007/BF00154722
25. Van Horn DLV, Schultz RO. Corneal preservation: Recent advances. Survey of Ophthalmol 1977;21(4):301:312
26. Lindstrom RL, Doughman DJ, Skelnik DL, Mindrup EA. Minnesota system corneal preservation. Br J Ophthalmol 1986;70(1);47-54. https://doi.org/10.1136/bjo.70.1.47
27. Pels E, Schuchard Y. The effects of high molecular weight dextran on the preservation of human corneas. Cornea. 1984/1985;3(3):219-227. https://doi.org/10.1007/s10792-007-9086-1
28. Pels E, Hilde B, Ilse C. Eye bank issues: II. preservation technique: warm versus cold storage. Int Ophthalmol. 2008;28(3):155-163. https://doi.org/10.1007/s10792-007-9086-1
29. Sperling S. Evaluation of the endothelium of human donor corneas by induced dilation of intercellular spaces and trypan blue. Greafes Arch Clin Exp Ophthalmol. 1986; 224(6):428–434. https://doi.org/10.1007/BF02173358
30. Thuret G, Manisolle C, Herrag S et al. Controlled study of the influence of storage medium type on endothelial assessment during corneal organ culture. Br J Ophthalmol 2004;88(4):579–581. https://doi.org/10.1136/bjo.2003.022020
31. Armitage WJ. Preservation of the cornea. Transfus Med Hemother 2011;38(2):143:147
32. Doughman DJ, Van Horn DL, Rodman W, Byrnes P, Lindstrom RL. Human corneal endothelial layer repair during organ culture. Arch Opthalmol. 1976;94(10):1791-1796. https://doi.org/10.1001/archopht.1976.03910040565016
33. Camposampiero D, Tiso R, Zanetti E, Ruzza A, Bruni A, Ponzin D. Improvement of human corneal endothelium in culture after prolonged hypothermic storage. Eur. J. Ophthalmol. 2003;13(9/10):745-751. PMid:14700093
34. Waller W, Van Horn DL: Electron microscopic study of the endothelium of stored and cryopreserved monkey corneas. Albrecht von Graefes Arch Klin Ophthalmol 1973;187:79-88. https://doi.org/10.1007/BF00444148
35. Van Horn DL, Schultz RO: Endothelial survival in cryopreserved human corneas: A scanning electron microscope study. Invest Ophthalmol Vis Sci.1974;13(1):7-16

Funding source: None
Conflicts of interest: None
Received on:
April 3, 2017.
Accepted on:
August 8, 2017.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados

 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket