

Ana Luiza Biancardi1; Aisa Lani2; Haroldo Vieira de Moraes Jr3
DOI: 10.17545/e-oftalmo.cbo/2015.42
ABSTRACT
The objective of this study was to establish evidence-based guidelines for the treatment of uveitis. The Brazilian Council of Ophthalmology, in partnership with the Brazilian Medical Association and the Brazilian Society of Uveitis, has created guidelines to standardize the procedures for the treatment of uveitis. We searched the Medline and Pubmed databases dated until August 2015 to find indications of intravitreal injections/implants and the use of immunosuppressants for the treatment of uveitis.
Keywords: Uveitis. Immunosuppressive Agents. Adrenal Cortex Hormones. Ttherapeutic Use.
RESUMO
Esta publicação tem como objetivo estabelecer diretrizes baseadas em evidências científicas para tratamento da uveíte. A necessidade de normatização de condutas em uveítes foi a principal motivação para o Conselho Brasileiro de Oftalmologia, em parceria com a Associação Médica Brasileira e Sociedade Brasileira de Uveíte, promover a elaboração das diretrizes. Foi realizada busca de evidência na base de informação científica Medline / Pubmed até agosto de 2015 para abordar as indicações de injeções / implantes intravítreos e uso de imunossupressores em uveítes.
Palavras-chave: Uveíte. Imunossupressores. Corticosteroides. Uso Terapêutico.
INTRODUCTION
Uveitis cases account for 2%-3% of ophthalmologic visits in emergency units; this limited presentation indicates that most ophthalmologists are not familiar with this condition.1,2
The Brazilian Council of Ophthalmology, in partnership with the Brazilian Medical Association and the Brazilian Society of Uveitis, has created guidelines to standardize the procedures for the treatment of uveitis.
Medical guidelines are implementable standards that assist in decision-making in clinical and surgical cases. These guidelines help standardize the safety of evidence-based procedures and professional ethics.
However, it is critical to emphasize that physician autonomy should be preserved.
METHODS
These guidelines were created after the analysis of relevant clinical complications associated with the treatment of uveitis. We searched for scientific information in the Medline and Pubmed databases dated until August 2015.
GUIDELINES
Our analysis indicated that oral and topical corticosteroids are the basis of treatment for most uveitis cases; however, prolonged use of oral corticosteroids causes undesirable and potentially severe side effects, which limits their use and warrants the adoption of alternative therapies. Prednisone doses ranging from 5.0 to 7.5 mg/day are considered physiological doses because they are compatible with the natural daily production of cortisol in the body. Other treatment strategies should be considered in patients requiring larger doses for prolonged periods in order to avoid adverse events, such as hypertension, diabetes mellitus, osteoporosis, hepatic steatosis, and pancreatitis. In addition, patients with these clinical conditions should avoid the prolonged use of oral corticosteroids.3,4 Therapeutic options for uveitis include intravitreal injections/implants and immunosuppressants.
1. DETAILS ON THE INTRAVITREAL INJECTION/IMPLANT OF CORTICOSTEROIDS:
1.1 They are a therapeutic option for the treatment of noninfectious unilateral posterior/intermediate uveitis for patients in whom treatment with systemic corticosteroids caused adverse events or in patients with contraindications to the prolonged use of systemic corticosteroids;5
1.2 They are a treatment option for patients with uveitis controlled with >10 mg/day prednisone for a prolonged period to avoid complications associated with the use of systemic corticosteroids;5
1.3 Injection of dexamethasone has been described as an adjuvant therapy in infectious cases provided that it is associated with intravitreal antibiotic therapy; examples include patients with toxoplasmic retinochoroiditis and patients who are either intolerant to or not eligible for the proposed treatment;6,7,8
1.4 They are used as an adjunctive therapy in endophthalmitis;9,10,11
1.5 Terapia adjuvante na endoftalmite.12,13
The two forms of administration of intravitreal corticosteroids are injection and slow-release implant. Table 1 summarizes the main features of intravitreal corticosteroids.5,14,15,16,17,18
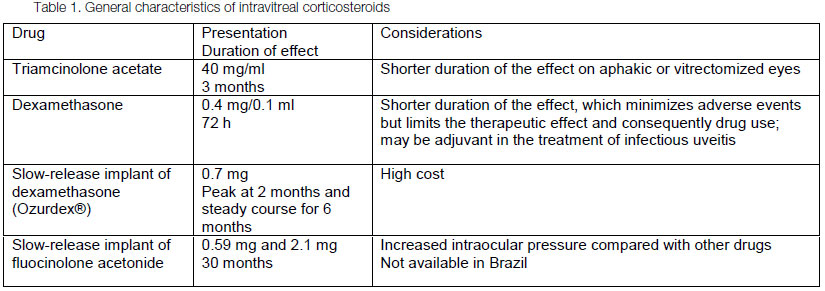
The complications due to intravitreal corticosteroids include ocular hypertension, cataract, retinal detachment, vitreous hemorrhage, endophthalmitis, crystalline lesion, and reactivation of infectious retinitis.5,19
Intraocular pressure (IOP) can be monitored 30 min after drug injection and at subsequent intervals that depend on the drug.
• After the use of triamcinolone: Assess IOP 1 week after treatment, every 2 weeks for the first month, and then monthly for up to 6 months.
• After the use of dexamethasone implant: Assess IOP 2 weeks after treatment, every 2 weeks in the first month, and then monthly for up to 6 months.
• After the use of fluocinolone acetonide implant: Assess IOP after 2 weeks of therapy, every 2 weeks in the first month, and then monthly up to 9 months.19
2. INTRAVITREAL INJECTION OF ANTI-VASCULAR ENDOTHELIAL GROWTH FACTOR (ANTI-VEGF) AGENTS
Anti-VEGF agents, such as ranibizumab (Lucentis®), bevacizumab (Avastin®), and aflibercept (Eylea®), are used in some uveitis cases but are considered off-label, meaning that its indication is not described in the prescription leaflet. Therefore, the patient should be informed about this and the physician should take responsibility for procedures involving these medications.
Some studies have reported the use of anti-VEGFs in patients with uveitis as a treatment option for macular edema that is unresponsive to corticosteroids and subretinal neovascular membranes. The use of anti-VEGFs has also been used for ischemic occlusive vasculitis, which stimulates the release of VEGFs; this complication occurs in patients with tuberculosis, Behçet's disease, sarcoidosis, and systemic lupus erythematosus, the latter of which is associated with photocoagulation.5,20,21,22,23,24,25,26,27
The advantages of anti-VEGFs compared with corticosteroids are the lower probability of complications, such as cataracts, increased intraocular pressure, retinal detachment, vitreous hemorrhage, and endophthalmitis.5
3. INTRAVITREAL INJECTION OF BIOLOGICAL AGENTS
Few studies have evaluated the intravitreal use of infliximab in patients with noninfectious uveitis, and the results are controversial. This lack of consistent scientific evidence limits the indication of this drug.5,28,29,30,31
4. USE OF IMMUNOSUPPRESSANTS3,4,32
Immunosuppressants are indicated for patients who have used high prednisone doses for more than 1 month or for those in whom there is absence of satisfactory control after 2–4 weeks of prednisone use.
They are also indicated for patients whose inflammatory status is controlled with high prednisone doses and for the suspension or reduction of prednisone to doses <10 mg/day after the management of uveitis. These cases include the following:
• Systemic diseases are chronic and may involve other organs and therefore may be treated with immunosuppressants to avoid complications associated with the prolonged use of prednisone at doses >10 mg/day. These diseases include Behçet's disease, Vogt–Koyanagi–Harada syndrome, sympathetic ophthalmia, severe cases of sarcoidosis, uveitis associated with seronegative spondyloarthropathies, and juvenile idiopathic arthritis.
• Sclerites, especially when associated with systemic diseases such as granulomatosis with polyangeitis
• Severe presentations of white dot syndromes such as serpiginous choroiditis and birdshot chorioretinopathy
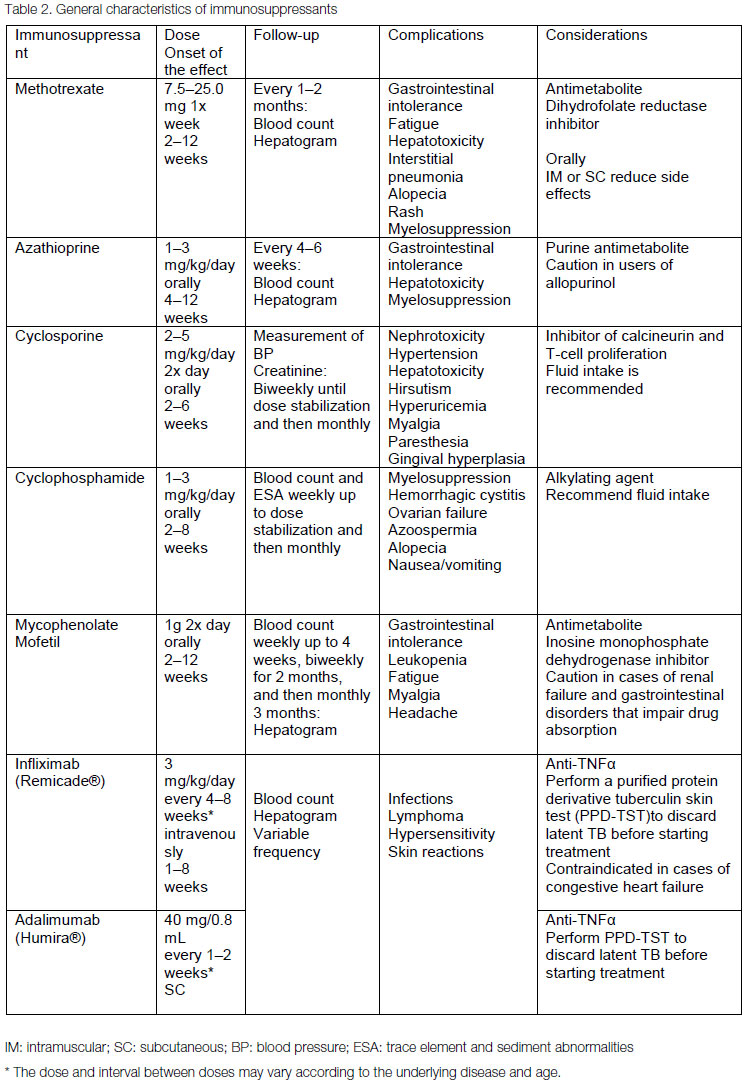
The choice of immunosuppressant depends on the patient's clinical condition and on any comorbidities or underlying diseases. Multidisciplinary follow-up with a rheumatologist or general practitioner is recommended to adequately monitor the patient's condition when uveitis is associated with chronic disease and to check for side effects. The corticosteroid dose should be gradually reduced 4–8 weeks after the introduction of the immunosuppressant.Os imunossupressores mais utilizados são metotrexato, azatioprina, ciclosporina, micofenolato mofetil, ciclosfosfamida e agentes biológicos (infliximabe e adalimumabe). O quadro 2 resume as principais características dos imunossupressores.
Promising biological agents for the treatment of noninfectious uveitis are rituximab (B-lymphocyte inhibitor), gevokizumab (monoclonal antibody that binds to IL-1β), and tocilizumab (anti-IL6 monoclonal antibody).32,33,34
CONCLUSIONS
Individualized treatment is critical for adequate control of uveitis, and no single therapy resolves all cases of the disease. A risk-benefit assessment should be performed for each therapeutic option. The choice of treatment depends on disease presentation, cause, and the patient's clinical condition. Although oral corticosteroids are widely used, chronic cases requiring long-term use or adverse events may prevent the continuation of this therapy, and the alternatives presented in this study should be considered. Although intravitreal treatments are advantageous because they prevent systemic adverse events, the use of immunosuppressants is indicated in bilateral cases and cases associated with systemic diseases. However, new biological agents should be used with caution; although their indication is well established in systemic autoimmune diseases, few studies to date have evaluated these drugs in the treatment of uveitis. Testing of uveitis treatments is limited by the rarity of the disease as research requires multicenter studies and recruitment of patients with noninfectious uveitis of different etiologies that may present distinct responses to treatment. Particular attention should be given to infectious etiologies that require associated antimicrobial coverage.
REFERENCES
1 Kaufman PLPLA, A.; Adler, F.H. Adler's physiology of the eye. 11 ed. ed: Elsevier; 2011.
2. Dua HS, Faraj LA, Said DG, Gray T, Lowe J. Human corneal anatomy redefined: a novel pre-Descemet's layer (Dua's layer). Ophthalmology. 013;120(9):1778-85. http://dx.doi.org/10.1016/j.ophtha.2013.01.018 PMid:23714320.
3. Straiko MD, Shamie N, Terry MA. Endothelial keratoplasty: past, present, and future directions. International ophthalmology clinics. 010;50(3):123-35. http://dx.doi.org/10.1097/IIO.0b013e3181e24746 PMid:20611023.
4. Mau K. What DSAEK is going on? An alternative to penetrating keratoplasty for endothelial dysfunction. Optometry. 2009;80(9):513-23. http://dx.doi.org/10.1016/j.optm.2008.11.010 PMid:19716079.
5. Talajic JC, Straiko MD, Terry MA. Descemet's stripping automated endothelial keratoplasty: then and now. International ophthalmology clinics. 2013;53(2):1-20. http://dx.doi.org/10.1097/IIO.0b013e31827eb6ba PMid:23470585.
6. Grottone GT, Pereira NC, Gomes JA. Endothelial keratoplasty: evolution and horizons. Arquivos brasileiros de oftalmologia. 2012;75(6):439-46. http://dx.doi.org/10.1590/S0004-27492012000600016 PMid:23715152.
7. Banitt MR, Chopra V. Descemet's stripping with automated endothelial keratoplasty and glaucoma. Current opinion in ophthalmology. 2010;21(2):144-9. http://dx.doi.org/10.1097/ICU.0b013e3283360b95 PMid:20040871.
8. Anshu A, Price MO, Tan DT, Price FW, Jr. Endothelial keratoplasty: a revolution in evolution. Survey of ophthalmology. 2012;57(3):236-52. http://dx.doi.org/10.1016/j.survophthal.2011.10.005 PMid:22516537.
9. Price MO, Price FW, Jr. Endothelial keratoplasty - a review. Clinical & experimental ophthalmology. 2010;38(2):128-40. http://dx.doi.org/10.1111/j.1442-9071.2010.02213.x PMid:20398103.
10. Giebel AW. DMEK: where less is more. International ophthalmology clinics. 2013;53(1):1-14. http://dx.doi.org/10.1097/IIO.0b013e31827744c4 PMid:23221881.
11. Hirlana Gomes Almeida ACDdS. Epidemiological profile of patients waiting for penetrating keratoplasty in state of Pernambuco - Brazil. Revista Brasileira de Oftalmologia. 2014;73(1).
12. Rose L, Kelliher C, Jun AS. Endothelial keratoplasty: historical perspectives, current techniques, future directions. Canadian journal of ophthalmology Journal canadien d'ophtalmologie. 2009;44(4):401-5. http://dx.doi.org/10.3129/i09-090 PMid:19606160.
13. Dapena I, Ham L, Melles GR. Endothelial keratoplasty: DSEK/DSAEK or DMEK- the thinner the better? Current opinion in ophthalmology. 2009;20(4):299-307. http://dx.doi.org/10.1097/ICU.0b013e32832b8d18 PMid:19417653.
14. Price MO, Price FW, Jr. Descemet's stripping with endothelial keratoplasty: comparative outcomes with microkeratome-dissected and manually dissected donor tissue. Ophthalmology. 2006;113(11):1936-42. http://dx.doi.org/10.1016/j.ophtha.2006.05.034 PMid:16935344.
15. Shinton AJ, Tsatsos M, Konstantopoulos A, Goverdhan S, Elsahn AF, Anderson DF, et al. Impact of graft thickness on visual acuity after Descemet's stripping endothelial keratoplasty. The British journal of ophthalmology. 2012;96(2):246-9. http://dx.doi.org/10.1136/bjophthalmol-2011-300462 PMid:22028474.
16. Taravella MJ, Shah V, Davidson R. Ultrathin DSAEK. International ophthalmology clinics. 2013;53(2):21-30. http://dx.doi.org/10.1097/IIO.0b013e31827823a8 PMid:23470586
17. Busin M, Madi S, Santorum P, Scorcia V, Beltz J. Ultrathin descemet's stripping automated endothelial keratoplasty with the microkeratome double-pass technique: two-year outcomes. Ophthalmology. 2013;120(6):1186-94. http://dx.doi.org/10.1016/j.ophtha.2012.11.030 PMid:23466268.
18. Yoeruek E, Bayyoud T, Hofmann J, Szurman P, Bartz-Schmidt KU. Comparison of pneumatic dissection and forceps dissection in Descemet membrane endothelial keratoplasty: histological and ultrastructural findings. Cornea. 2012;31(8):920-5. http://dx.doi.org/10.1097/ICO.0b013e31823f7870 PMid:22511023.
19. Guerra FP, Anshu A, Price MO, Price FW. Endothelial keratoplasty: fellow eyes comparison of Descemet stripping automated endothelial keratoplasty and Descemet membrane endothelial keratoplasty. Cornea. 2011;30(12):1382-6. http://dx.doi.org/10.1097/ICO.0b013e31821ddd25 PMid:21993468.
20. Feng MT, Price MO, Price FW, Jr. Update on Descemet membrane endothelial keratoplasty (DMEK). International ophthalmology clinics. 2013;53(2):31-45. http://dx.doi.org/10.1097/IIO.0b013e31827822b9 PMid:23470587.
21. Tourtas T, Laaser K, Bachmann BO, Cursiefen C, Kruse FE. Descemet membrane endothelial keratoplasty versus descemet stripping automated endothelial keratoplasty. American journal of ophthalmology. 2012;153(6):1082-90 e2.
22. Maier AK, Gundlach E, Gonnermann J, Klamann MK, Eulufi C, Bertelmann E, et al. Fellow Eye Comparison of Descemet Membrane Endothelial Keratoplasty and Penetrating Keratoplasty. Cornea. 2013. http://dx.doi.org/10.1097/ICO.0b013e31829dd816 PMid:23928950.
23. Armour RL, Ousley PJ, Wall J, Hoar K, Stoeger C, Terry MA. Endothelial keratoplasty using donor tissue not suitable for full-thickness penetrating keratoplasty. Cornea. 2007;26(5):515-9. PMid:17525642.
24. Phillips PM, Terry MA, Shamie N, Chen ES, Hoar KL, Stoeger C, et al. Descemet's stripping automated endothelial keratoplasty (DSAEK) using corneal donor tissue not acceptable for use in penetrating keratoplasty as a result of anterior stromal scars, pterygia, and previous corneal refractive surgical procedures. Cornea. 2009;28(8):871-6. http://dx.doi.org/10.1097/ICO.0b013e318199f8d7 PMid:19654530.
25. Moshirfar M, Khalifa YM, Davis D, Fenzl CR, Espandar L, Chang JC, et al. Descemet stripping automated endothelial keratoplasty using donor corneas with previous laser in situ keratomileusis or photorefractive keratectomy: a case series and donor cap histopathology. Cornea. 2012;31(5):533-7. http://dx.doi.org/10.1097/ICO.0b013e31820142be PMid:21993455.
26. Khor WB, Teo KY, Mehta JS, Tan DT. Descemet stripping automated endothelial keratoplasty in complex eyes: results with a donor insertion device. Cornea. 2013;32(8):1063-8. http://dx.doi.org/10.1097/ICO.0b013e31828321f8 PMid:23449486.
27. Eguchi H, Miyamoto T, Hotta F, Tomida M, Inoue M, Mitamura Y. Descemet-stripping automated endothelial keratoplasty for vitrectomized cases with traumatic aniridia and aphakic bullous keratopathy. Clinical ophthalmology. 2012;6:1513-8. PMid:23055672 PMCid:PMC3460703.
28. Price MO, Price FW, Jr., Trespalacios R. Endothelial keratoplasty technique for aniridic aphakic eyes. Journal of cataract and refractive surgery. 2007;33(3):376-9. http://dx.doi.org/10.1016/j.jcrs.2006.10.052 PMid:17321384.
29. Busin M, Beltz J, Scorcia V. Descemet-stripping automated endothelial keratoplasty for congenital hereditary endothelial dystrophy. Archives of ophthalmology. 2011;129(9): 1140-6. http://dx.doi.org/10.1001/archophthalmol.2011.114 PMid:21555597.
30. Anwar HM, El Danasoury A, Hashem A. Descemet's stripping automated endothelial keratoplasty for congenital hereditary endothelial dystrophy. Clinical ophthalmology. 2012;6:159-63. http://dx.doi.org/10.2147/OPTH.S28405 PMid:22291459 PMCid:PMC3267538.
31. Hashemi H, Ghaffari R, Mohebi M. Posterior lamellar keratoplasty (DSAEK) in Peters anomaly. Cornea. 2012;31(10):1201-5. http://dx.doi.org/10.1097/ICO.0b013e31825697a4 PMid:22790185.
32. Covert DJ, Koenig SB. Descemet stripping and automated endothelial keratoplasty (DSAEK) in eyes with failed penetrating keratoplasty. Cornea. 2007;26(6):692-6. http://dx.doi.org/10.1097/ICO.0b013e31805fc38f PMid:17592318.
33. Straiko MD, Terry MA, Shamie N. Descemet stripping automated endothelial keratoplasty under failed penetrating keratoplasty: a surgical strategy to minimize complications. American journal of ophthalmology. 2011;151(2):233-7 e2.
34. Graue-Hernandez EO, Zuniga-Gonzalez I, Hernandez-Camarena JC, Jaimes M, Chirinos-Saldana P, Navas A, et al. Tectonic DSAEK for the Management of Impending Corneal Perforation. Case reports in ophthalmological medicine. 2012;2012:916528. http://dx.doi.org/10.1155/2012/916528 PMid:23259100 PMCid:PMC3521400.
Source of funding: None declared
Conflict of interests: None declared
REC Opinion: Does not apply
Received on:
November 15, 2015.
Accepted on:
December 1, 2015.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket