

Leopoldo Ernesto Oiticica Barbosa
DOI: 10.17545/eOftalmo/2025.0008
Este artigo pertence à Edição Especial SLT no Glaucoma: Da Prática Clínica à Perspectiva de Implementação no SUS
ABSTRACT
The growing demand for eye care poses significant challenges to the sustainability of public health systems, especially in the management of glaucoma, a chronic, silent disease with a high socioeconomic impact. This article analyzes blindness from a health economics perspective and discusses international and national evidence supporting a shift from a model centered on the continuous use of eye drops to early intervention strategies. Based on clinical studies, cost-effectiveness analyses, and the experience of the Unified Health System, we explore the role of selective laser trabeculoplasty as a clinically effective, economically viable, and socially equitable alternative and indicate pathways for its structured incorporation into the Unified Health System.
Keywords: Glaucoma; Selective laser trabeculoplasty; Cost-effectiveness; Unified Health System.
RESUMO
A crescente demanda por cuidados oftalmológicos impõe desafios relevantes à sustentabilidade dos sistemas públicos de saúde, especialmente no manejo do glaucoma, uma doença crônica, silenciosa e de alto impacto socioeconômico. Este artigo analisa a cegueira sob a perspectiva da economia da saúde, discutindo evidências internacionais e nacionais que sustentam a mudança do modelo centrado no uso contínuo de colírios para estratégias de intervenção precoce. A partir de estudos clínicos, análises de custo-efetividade e da experiência do Sistema Único de Saúde, o texto explora o papel da trabeculoplastia seletiva a laser como alternativa clinicamente eficaz, economicamente viável e socialmente equitativa, apontando caminhos para sua incorporação estruturada no Sistema Único de Saúde.
Palavras-chave: Glaucoma; Trabeculoplastia seletiva a laser; Custo-efetividade; Sistema Único de Saúde.
INTRODUCTION
The cost of blindness and the imperative of sustainability
Often, the focus of the ophthalmology community is on debating the technical refinements of phacoemulsification or the futuristic promises of gene therapy. However, it is imperative that we turn our attention to an equally vital but structural issue: health economics and the sustainability of public ophthalmology. It is no exaggeration to say that eye health today stands at the critical intersection between accelerated technological progress and the challenge of universal access.
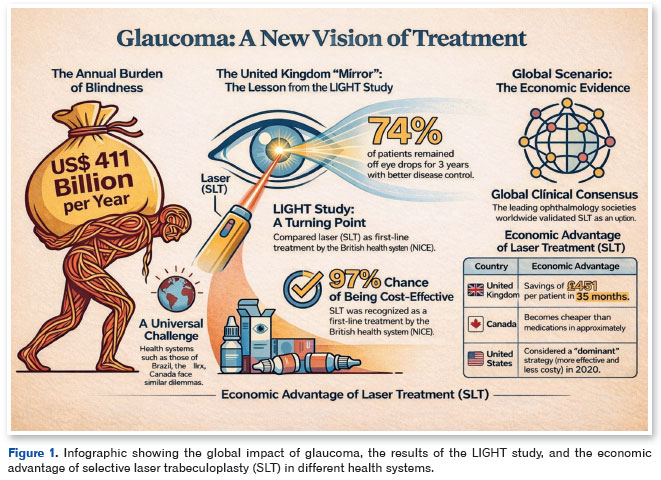
We know that vision loss transcends personal tragedy; it represents a massive global economic burden. Productivity losses due to blindness and visual impairment are estimated to amount to US$ 411 billion per year worldwide1. Therefore, discussing cost-effectiveness and resource allocation does not mean reducing medicine to cold numbers but rather guaranteeing visual dignity to as many patients as possible within health systems that operate with finite resources.
To understand the scenario of our Unified Health System (SUS), we need to look outward. Brazil is not alone in facing this challenge; global public health systems encounter similar dilemmas that mirror our reality. Comparative analyses of health systems, particularly those of the United Kingdom, Canada, and Australia, show that the pressure for allocative efficiency is a universal constant2,3.
The UK "mirror": lessons from the LiGHT study and the NHS
The United Kingdom's National Health Service (NHS) is often used as a reference because of its public and universal nature, which resembles the principles of the SUS. There, ophthalmology has become the busiest outpatient specialty, accounting for almost 10% of the entire patient waiting list4. The NHS offers a hard lesson about the bottleneck created by chronic treatment: despite free access, repressed demand has led to very long waiting lists.
More alarming for our reality is the concept of the "hidden waiting list" for follow-up appointments, in which patients with glaucoma—a silent and progressive disease—run the risk of losing their sight while waiting for their prescriptions to be renewed or their therapy to be adjusted4,5. The traditional model, which depends on patient adherence to the daily use of eye drops and frequent visits to measure intraocular pressure (IOP), has proved unsustainable in an aging population.
It was in this context of care pressure that the LiGHT(Laser in Glaucoma and Ocular Hypertension Trial) study began. This multicenter, randomized clinical trial not only challenged clinical conventions but also shook the foundations of public resource allocation by comparing primary selective laser trabeculoplasty (SLT) with conventional treatment using eye drops (prostaglandin analogs) in treatment-naive patients.
The 6-year results of LiGHT have been conclusive and provide technical guidance for health management6,7:
• Superior pressure control: SLT has been shown to be as effective or more effective than medication, with better long-term visual field preservation and a reduced need for incisional glaucoma surgery (trabeculectomy).
• Independence from medication: A significant proportion (74%) of patients initially treated with SLT did not require eye drops to control IOP in the first 3 years, mitigating the serious issues of nonadherence and ocular surface side effects.
• Cost-effectiveness: SLT was 97% more likely to be cost-effective for the NHS than eye drops6.
Given this evidence, the National Institute for Health and Care Excellence (NICE) updated its guideline (NG81) in 2022, recommending SLT as the first-line treatment for ocular hypertension and open-angle glaucoma8.
The global scenario: clinical consensus and economic proof
The paradigm shift promoted by LiGHT has reverberated worldwide, with its efficacy validated across different clinical settings. This robust evidence has aligned the guidelines of the American Academy of Ophthalmology, the European Glaucoma Society, and, importantly, the Brazilian Glaucoma Society (SBG). The current consensus is clear: SLT should be considered a first-choice strategy rather than a secondary alternative following eye drop failure9.
This global validation is supported by a series of cost-effectiveness studies that consistently demonstrate the long-term economic advantage of laser over polypharmacy:
• United Kingdom (NHS): The economic analysis of the LiGHT study showed that a laser-first strategy generated an average saving of £451 (pounds sterling) per patient at 36 months, reducing costs associated with salvage incisional surgeries and multiple follow-up appointments5.
• United States (Medicare): Using Markov models to simulate glaucoma progression over 20 years, Stein et al. demonstrated that initial laser treatment generates significant savings compared with monotherapy with prostaglandin analogs, identifying laser as the "dominant" strategy with favorable incremental cost-effectiveness ratio values10.
• Canada (OHIP): Within the Ontario public system, Lee and Hutnik projected accumulated costs over 6 years, showing that SLT becomes cheaper than most branded drug combinations within 1 year. Even compared with cheaper generics, laser treatment reaches its financial break-even point between 13 and 40 months, representing net savings for the system thereafter11 (Figure 1).
• New Zealand: A cost-minimization analysis by Ngan et al. reinforced that, in a public system with limited resources, SLT is superior even to subsidized drug treatments12.
However, clinical acceptance and economic evidence do not automatically eliminate management barriers. Canada's health system provides a guideline similar to that of Brazil. In the province of British Columbia, for example, although health technology assessments recognize the value of the procedure, the actual provision of SLT is hindered by practical obstacles. Reports indicate that care is often limited by the capital costs of equipment acquisition and the rigidity of hospital budget allocations13. This difficulty in translating "theoretical coverage" into "practical access" is exactly what creates the bottleneck in our country.
The Brazilian reality: local evidence and the funding maze
When we look to Brazil, the question is inevitable: if SLT is clinically superior and economically advantageous, why is it still not the standard treatment in the SUS?
The answer does not lie in a lack of evidence. Recent national literature unanimously highlights the advantages of this technology. Tavares et al. conducted a robust budget impact analysis for the SUS, demonstrating that SLT has a significantly lower economic impact than clinical treatment with timolol and prostaglandin analogs at both 1 and 5 years after treatment. Projections indicate potential savings of billions of Brazilian reais, depending on the adoption of the technology14. In line with these findings, Gravina et al., using Markov models, concluded that initiating treatment with SLT is a dominant strategy (more effective and less costly) than eye drops, because it provides higher quality-adjusted life years for the patient15.
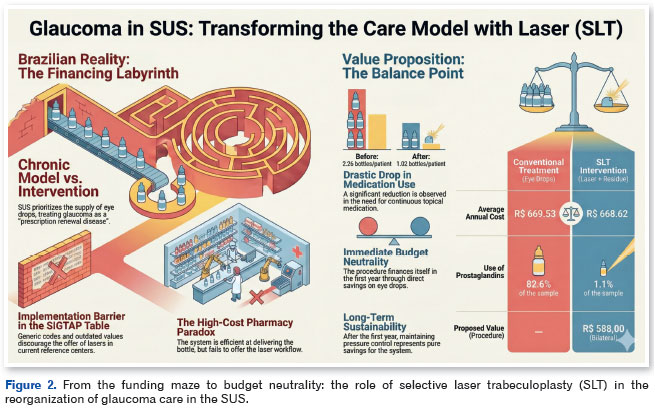
However, we face a complex implementation barrier: the funding architecture. Currently, the SUS Glaucoma Program favors drug treatment. The system efficiently provides medication through the "High Cost Pharmacy" ("Farmácia de Alto Custo" in Portuguese) but does not have a pathway designed to offer laser treatment as first-line therapy16. There is no exclusive coding for SLT in the SIGTAP Table. Its current use in practice relies on nonspecific codes and transfers that are incompatible with the operating costs of the equipment, resulting in underfunding that discourages specialized services from adopting the technology.
Unlike cataract, which benefits from a high-productivity flow financed through FAEC or the MAC ceiling and supports a large volume of surgeries17, glaucoma remains trapped in a "chronic maintenance" model. While other countries have invested in infrastructure to decongest outpatient clinics, Brazil is still struggling to transform glaucoma from a "prescription renewal" disease into an "early intervention" one.
The value proposition: The "balance point" for the SUS
To overcome the obstacle posed by the SIGTAP Table, it is necessary to present a pragmatic value proposition based on "real-life" data. In this context, we recently published a proposal for a viable path forward.
In a prospective interventional clinical study conducted within the SUS, replacing eye drops with SLT resulted in a significant reduction in the need for medication after 12 months: the average number of vials per patient decreased from 2.26 to 1.02, with a marked reduction in the use of prostaglandin analogs (from 82.6% to 1.1% of the sample), which are the most costly medications for the government18.
Based on these data, it was possible to calculate the break-even point. While the reference group (conventional treatment) had an average annual medication cost of R$669.53 per patient, the post-SLT group's residual expense fell to R$80.62. These savings allowed the proposal of a price of R$588.00 for the bilateral SLT procedure19. Thus, the total annual cost of the intervention group (including the procedure plus residual medication) is R$668.62, ensuring budget neutrality compared with conventional treatment in the first year (Figure 2).
This logic is powerful for public management for three reasons:
1. Immediate budget neutrality: The introduction of the procedure is practically self-funding in the first year, as it is covered by direct savings from reduced use of eye drops.
2. Long-term savings: Because SLT has a lasting effect, subsequent years of treatment represent a net saving for the system.
3. Feasibility: The proposed price makes it feasible for accredited centers to acquire and maintain the technology.
Conclusion: The role of the ophthalmologist and the manager
In view of the above, the technical conclusion is clear, but the practical application of SLT requires a review of care pathways. Officially, first-line SLT is still not the predominant practice in the SUS, which continues to prioritize medication.
However, data from the LiGHT study, international experience, and Brazilian evidence demonstrate that we now have a golden opportunity. Transitioning to SLT not only preserves the ocular surface and improves patients' quality of life but also serves as a tool for social equity. In a country with vast regional disparities20, a single procedure that ensures IOP control represents an intervention with high social impact.
The future of public ophthalmology demands that specialists move beyond merely prescribing eye drops and become interventional glaucoma physicians. Science has already provided the path and the economic model; now it is up to public management to pave the way.
REFERENCES
1. Burton MJ, Ramke J, Marques AP, Bourne RRA, Congdon N, Jones I, et al. The Lancet Global Health Commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551.
2. OECD. Institutionalising Health Accounts in Brazil: A Review of Methods, Data and Policy Relevance. OECD Reviews of Health Systems. Paris: OECD Publishing; 2025. Disponível em: https://www.oecd.org/en/publications/institutionalising-health-accounts-in-brazil_b6d405f9-en.html
3. Dixit SK, Sambasivan M. A review of the Australian healthcare system: A policy perspective. SAGE Open Med. 2018 Apr 12;6:2050312118769211.
4. The Royal College of Ophthalmologists. The Way Forward: Glaucoma. London: RCOphth; 2017.
5. Gazzard G, Konstantakopoulou E, Garway-Heath D, Garg A, Vickerstaff V, Hunter R, Ambler G, Bunce C, Wormald R, Nathwani N, Barton K, Rubin G, Buszewicz M; LiGHT Trial Study Group. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505–1516.
6. Gazzard G, Konstantakopoulou E, Garway-Heath D, Adeleke M, Vickerstaff V, Ambler G, Hunter R, Bunce C, Nathwani N, Barton K; LiGHT Trial Study Group. LiGHT trial: 6-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139-151.
7. Wright DM, Konstantakopoulou E, Montesano G, Nathwani N, Garg A, Garway-Heath D, et al. Visual Field Outcomes from the Multicenter, Randomized Controlled Laser in Glaucoma and Ocular Hypertension Trial (LiGHT). Ophthalmology. 2020; 127(10):1313-1321.
8. National Institute for Health and Care Excellence (NICE). Glaucoma: diagnosis and management. NICE guideline [NG81]. London: NICE; 2017 (updated 2022). Disponível em: https://www.nice.org.uk/guidance/ng81
9. Narayanaswamy A, Sood SR, Thakur S. Selective laser trabeculoplasty: An updated narrative review. Indian J Ophthalmol. 2024; 72(3):312-319.
10. Stein JD, Kim DD, Peck WW, Giannetti SM, Hutton DW. Cost-effectiveness of medications compared with laser trabeculoplasty in patients with newly diagnosed open-angle glaucoma. Arch Ophthalmol. 2012;130(4):497-505.
11. Lee R, Hutnik CM. Projected cost comparison of selective laser trabeculoplasty versus glaucoma medication in the Ontario Health Insurance Plan. Can J Ophthalmol. 2006;41(4):449-56.
12. Ngan K, Fraser E, Buller S, Buller A. A cost minimisation analysis comparing iStent accompanying cataract surgery and selective laser trabeculoplasty versus topical glaucoma medications in a public healthcare setting in New Zealand. Graefes Arch Clin Exp Ophthalmol. 2018;256(11):2181-2189.
13. Health Technology Assessment Report. Effectiveness and cost-effectiveness of minimally invasive glaucoma surgery in patients with glaucoma in British Columbia. British Columbia Health Technology Assessment Committee; 2020.
14. Tavares IM, Hirai FE, Landim DFC, Zucchi P. Initial Treatment of Glaucoma with Selective Laser Trabeculoplasty: Economic Impact from the Perspective of the Brazilian Public Health System. medRxiv. 2024. doi:10.1101/2024.07.21.24310769
15. Gravina DM, Guedes RA, Chaoubah A. Custo-utilidade do tratamento primário não farmacológico do glaucoma de ângulo aberto. Rev Bras Oftalmol. 2023;82:e0011.
16. Brasil. Ministério da Saúde. Protocolo Clínico e Diretrizes Terapêuticas do Glaucoma. Brasília: Ministério da Saúde; 2013.
17. Fernandes AG, Ferraz AN, Lemos RS, Watanabe SES, Berezovsky A, Salomão SR. Trends in cataract surgical treatment within the Brazilian national public health system over a 20-year period: Implications for Universal Eye Health as a global public health goal. PLOS Glob Public Health. 2022;2(6):e0000328.
18. Barbosa LEO, Barboza WL, Guedes RP, Pereira CR, Susanna R Jr, Hatanaka M. Selective Laser Trabeculoplasty as a Substitute for Medications in Patients with Mild-to-moderate Glaucoma in the Brazilian Public Health System. J Glaucoma. 2024;33(5):303-309.
19. Barbosa LEO, Barboza WL, Guedes RAP, Chaoubah A, Hatanaka M. Cost-effectiveness of selective laser trabeculoplasty as a replacement for hypotensive eye drops in the Brazilian public health system. Clinics (São Paulo). 2025 Apr 23:80:100650.
20. Scheffer M, Moreira JPL, Bahia L, Borges SAM, Cassenote AJF, Gameiro GR, et al. Regional inequalities in the supply of ophthalmologists and the volume of cataract surgeries between the public and private health sectors in Brazil. Arq Bras Oftalmol. 2026;89(1):e2025-0218.
AUTHOR INFORMATION

Funding: No specific financial support was available for this study
Conflict of interest: None of the authors have any potential conflict of interest to disclose
Received on:
February 3, 2026.
Accepted on:
February 4, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket