

Diogo Gonçalves dos Santos Martins1; Paulo Schor1; Eduardo Damasceno2; Thiago Gonçalves dos Santos Martins3
DOI: 10.17545/eOftalmo/2025.0003
ABSTRACT
This article addresses the diversity and impact of arboviruses in Central and South America, with a particular focus on the Oropouche virus, the causative agent of Oropouche fever. The Amazon region is highlighted as an area of high viral diversity, with recurrent outbreaks of mosquito-borne diseases such as chikungunya, dengue, Zika, and West Nile fever. The ophthalmological manifestations associated with these arboviruses are discussed, ranging from mild symptoms such as photophobia and ocular pain to severe conditions including retinitis and uveitis. Oropouche fever is identified as an emerging public health concern, with a substantial increase in reported cases in Brazil in recent years, underscoring the urgent need for vaccine development and effective control strategies. The article emphasizes the importance of epidemiological surveillance and examines the roles of climate change and increased human mobility in facilitating viral dissemination. In addition, challenges related to the diagnosis and clinical management of arboviral infections with ocular involvement are highlighted.
Keywords: Chikungunya; Dengue; Ophthalmological manifestations; Mayaro Fever; Oropuche fever; West Nile fever; Zika; Zoonoses.
RESUMO
Este artigo aborda a diversidade e os impactos dos arbovírus na América Central e do Sul, com foco no vírus Oropouche, responsável pela febre do Oropouche. A região amazônica é destacada como uma área de alta diversidade viral, com surtos recorrentes de doenças transmitidas por mosquitos, como Chikungunya, dengue, Zika e febre do Nilo Ocidental. O artigo também discute as manifestações oftalmológicas associadas a esses vírus, incluindo fotofobia, dor ocular e condições mais graves, como retinite e uveíte. O Oropouche é identificado como uma ameaça crescente à saúde pública, com número significativo de casos recentes no Brasil, e ressalta-se a necessidade de desenvolvimento de vacinas para conter sua disseminação. O texto enfatiza a importância da vigilância epidemiológica, o impacto do aquecimento global e do aumento da mobilidade humana na disseminação desses vírus, bem como os desafios no diagnóstico e tratamento dessas doenças.
Palavras-chave: Febre do Oropouche; Zoonoses; Manifestações oftalmológicas; Dengue; Zika; Chikungunya; Febre do Nilo Ocidental; Febre Mayaro.
INTRODUCTION
Central and South America are critical regions for the emergence of zoonotic diseases1. In the Brazilian Amazon, between 1954 and 1988, 187 distinct virus species were isolated from mammals (including humans) and mosquitoes2. More recent studies continue to confirm the high diversity of arboviral pathogens circulating in South America3. Although not all newly identified viruses are pathogenic, these findings underscore the remarkable viral diversity of the Neotropical region and its predisposition to the emergence of arboviral diseases.
Active epidemiological surveillance, including systemic sample collection through scheduled surveys, has identified the circulation of at least five viruses belonging to the Peribunyaviridae family in Brazil2, among which the Oropouche virus is responsible for Oropouche fever. Concern regarding this infection intensified following a warning issued by the Pan American Health Organization on February 2, 2024, highlighting the increasing number of cases worldwide2. Epidemiological data have revealed warning signs of disease expansion within Brazil, with a notable rise in cases in 2022 and 2024 associated with the emergence of a new recombinant viral strain2. Despite these developments, knowledge regarding the natural history and clinical spectrum of Oropouche fever remains limited.
Mammals and wild birds serve as natural reservoirs of the Oropouche virus. Owing to the broad geographic distribution and migratory capacity of birds, outbreaks may occur even in remote areas, provided that competent vectors and susceptible hosts are present at sufficient densities4. Mammalian reservoirs include sloths, primates, and rodents. Humans infected in forested environments may act as "bridge hosts," facilitating viral transmission from sylvatic cycles to urban settings. In urban and peri-urban environments, Culicoides paraensis is the primary vector responsible for viral propagation and maintenance, leading to large-scale epidemics in densely populated areas5. During outbreaks, domestic animals, such as chickens, have been proposed as potential amplifying hosts, contributing to increased viral prevalence6.
Culex quinquefasciatus has also been identified as a competent vector for Oropouche virus during outbreaks in Brazil, a finding later confirmed under laboratory conditions, where infected mosquitoes successfully transmitted the virus to healthy hamsters6. Given the wide geographic distribution of Cx. quinquefasciatus, there is a concern that Oropouche virus may expand beyond the Americas to regions such as Africa, Australia, or Southeast Asia.
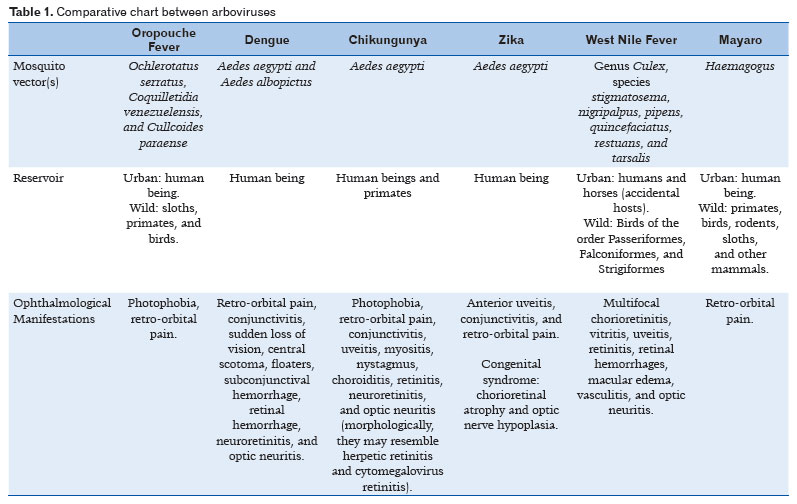
In this context, this narrative review aims to summarize the ophthalmological manifestations associated with Oropouche fever and to discuss its principal differential diagnoses, particularly in relation to other arboviral infections of ophthalmological relevance. By synthesizing current evidence and comparing ocular involvement across Oropouche, dengue, Zika, chikungunya, West Nile, and Mayaro virus infections, this review seeks to support ophthalmologists and clinicians in the early recognition, differential diagnosis, and clinical management of emerging arboviral diseases with ocular involvement.
The purpose of this study is to provide a comprehensive narrative review of the ophthalmological manifestations associated with Oropouche fever and to discuss its principal differential diagnoses, with particular emphasis on other arboviral infections of ophthalmological relevance. By synthesizing current evidence on ocular involvement in Oropouche virus infection and comparing these findings with those reported for well-established arboviruses—including dengue, Zika, Chikungunya, West Nile, and Mayaro viruses—this review aims to assist ophthalmologists and clinicians in the early recognition, accurate differential diagnosis, and appropriate clinical management of emerging arboviral diseases with ocular involvement.
METHODS
A narrative literature review was conducted to examine published studies addressing the epidemiology, clinical characteristics, and ophthalmological manifestations of Oropouche fever and other relevant arboviral infections. Scientific articles, review papers, and epidemiological reports were identified through searches of major biomedical databases, including PubMed and SciELO, as well as publications from public health organizations. Reference selection prioritized studies reporting ocular findings, neuro-ophthalmological involvement, and differential diagnostic considerations among arboviral diseases. Given the descriptive nature of this review, no restrictions were applied with respect to study design. The retrieved findings were qualitatively synthesized to provide an integrated overview of the ophthalmological manifestations associated with emerging arboviral infections.
DISCUSSION
Ophthalmological manifestations
Oropuche fever
Oropouche fever has an incubation period of approximately 3–10 days and typically presents as an acute, self-limiting febrile illness. Reported ophthalmological manifestations include photophobia, retro-orbital pain, and hemorrhagic findings such as petechiae. In most symptomatic individuals, clinical recovery occurs spontaneously within approximately seven days6. However, the detection of Oropouche virus (OROV) RNA in the cerebrospinal fluid of patients from Amazonas State provides evidence of potential central nervous system involvement during outbreaks. Correspondingly, cases of aseptic meningitis and meningoencephalitis have been described, although fatal outcomes in adults remain uncommon7.
Recent outbreaks in Brazil have substantially expanded the recognized clinical spectrum of Oropouche fever by demonstrating vertical transmission and severe congenital disease. Serologically confirmed maternal–fetal OROV infection has been associated with fetal loss and profound neurodevelopmental impairment. Newborns from the Brazilian Amazon, born to mothers who experienced systemic febrile illness during pregnancy, have presented with severe microcephaly, arthrogryposis, and extensive abnormalities of the brain and spinal cord on neuroimaging, including cerebral atrophy and major structural malformations. Fundoscopic examinationin affected infants has revealed macular chorioretinal scars, focal pigmentary alterations, and attenuation of retinal vessels. Although congenital OROV infection shares several clinical features with congenital Zika syndrome, distinct neuroimaging findings and neurological characteristics support the recognition of a specific congenital syndrome related to in utero OROV exposure8.
Chikungunya
Chikungunya is an alphavirus belonging to the Togaviridae family and is transmitted primarily by Aedes aegypti and Aedes albopictus mosquitoes. The term "Chikungunya," meaning "that which bends," during the 1952–1953 outbreak in Tanzania, reflects the severe arthralgia characteristic of the disease9. Ophthalmological manifestations include photophobia, retrobulbar pain, and conjunctivitis. More severe ocular involvement has been reported, including hypertensive uveitis, nystagmus, and myositis10. Retinal involvement may manifest as choroiditis, retinitis, neuroretinitis, or optic neuritis, with clinical and morphological features that may resemble herpetic or cytomegalovirus retinitis, complicating differential diagnosis10.
Dengue
Dengue is the most prevalent flaviviral disease worldwide and is caused by a single-stranded RNA virus with four serotypes (DENV-1–DENV-4), transmitted mainly by A. aegypti and A. albopictus. Ocular manifestations are diverse and include sudden visual loss, central scotoma, floaters, subconjunctival hemorrhage, retinal hemorrhage, neuroretinitis, and optic neuritis. Retro-orbital pain and conjunctivitis are frequently observed during the acute febrile phase11.
Retinal hemorrhages have emerged as a particularly important ocular complication of dengue fever, often occurring during defervescence and coinciding with the nadir of thrombocytopenia. Fundoscopic findings may include macular hemorrhages associated with exudative maculopathy, which can contribute to visual impairment even when not directly responsible for visual symptoms. Dengue maculopathy represents a clinically significant entity characterized by acute central vision loss and distinct optical coherence tomography patterns, including diffuse retinal thickening, cystoid macular edema, and foveolitis. Additional reported manifestations include cotton wool spots, retinal vasculitis, exudative retinal detachment, and anterior uveitis, underscoring the wide spectrum of ophthalmic involvement and the importance of ophthalmological assessment in dengue patients presenting with visual complaints12.
Zika virus
Zika virus, a flavivirus first identified in rhesus monkeys in Uganda's Zika Forest in 1947, is transmitted primarily by A. aegypti. In addition to vector-borne transmission, sexual, perinatal, and blood transfusion transmission–related transmission have been documented. The most severe consequences occur when infection affects pregnant women, particularly during the first trimester, leading to congenital Zika syndrome. This syndrome is characterized by microcephaly, sensorineural hearing loss, and ocular abnormalities such as chorioretinal atrophy and optic nerve hypoplasia. In adults, Zika virus infection is generally mild but may be associated with conjunctivitis, anterior uveitis, and retro-orbital pain13-15.
West Nile fever
West Nile virus, an RNA flavivirus transmitted primarily by Culex mosquitoes, was first identified in New York in 1999 and has since affected more than 3 million individuals in the United States. The infection may result in neuroinvasive disease, including meningitis, encephalitis, and acute flaccid paralysis. Ocular manifestations are relatively common, particularly in patients with neurological involvement, and include multifocal chorioretinitis and vitreous inflammation. Additional findings include uveitis, retinitis, retinal hemorrhages, macular edema, retinal vasculitis, and optic neuritis. Visual disturbances are more frequently observed in patients who develop encephalitis16.
Mayaro fever
Mayaro fever is an acute febrile illness caused by the Mayaro virus, an arbovirus of the Togaviridae family transmitted primarily by wild mosquitoes of the Haemagogus genus. First isolated in Trinidad in 1954, the virus was subsequently identified in Brazil in 1955 along the Guamá River near Belém, Pará. Since then, sporadic cases and localized outbreaks have been reported throughout the Americas, particularly in the Amazon region and in northern and central-western Brazil.
The clinical presentation of Mayaro fever closely resembles that of chikungunya and other arboviral infections, with abrupt onset of high fever (39°C–40°C), headache, arthralgia, myalgia, joint swelling, chills, malaise, and rash (exanthema). Gastrointestinal symptoms such as vomiting and diarrhea are common, and additional manifestations may include nausea, cough, sore throat, abdominal pain, nasal congestion, pruritus, anorexia, lymphadenopathy, and gingival bleeding. Ophthalmological manifestations are less frequently reported but may include retro-orbital pain (Table 1)17.
The eye is an immune-privileged organ, possessing specialized anatomical and immunological mechanisms that limit inflammatory responses to preserve visual function. While this immune privilege protects ocular tissues from immune-mediated damage, it may also permit viral persistence within ocular compartments, enabling pathogens to evade systemic immune clearance. Emerging evidence has demonstrated the prolonged presence of viral genetic material in ocular fluids, as illustrated by the detection of Mpox virus in conjunctival and intraocular samples after systemic resolution of infection. This phenomenon highlights the potential role of the eye as a viral reservoir, particularly in emerging and reemerging arboviral diseases. Infections such as dengue, Zika, and potentially Oropouche virus may exploit this immune environment, contributing to delayed or atypical ocular manifestations and reinforcing the need for ophthalmological surveillance during and after systemic viral illness18.
Arboviruses are distributed globally, except Antarctica, and their clinical diagnosis remains challenging due to overlapping systemic and ocular manifestations and the absence of specific antiviral therapies. In this context, recognition of ophthalmological findings is critical for accurate diagnosis, appropriate clinical follow-up, and prevention of long-term visual sequelae.
Oropouche virus represents a growing public health concern in South America, where it causes sustained endemic transmission and recurrent outbreaks yet remains neglected due to its clinical similarity to other arboviral infections, particularly dengue. Limited epidemiological data regarding its true distribution, prevalence, and incidence in humans, animal reservoirs, and vectors further hinder effective surveillance. The recent expansion of Oropouche fever is likely driven by ecological disruption, climate change, and increased human mobility. These factors underscore the urgent need for strengthened public health strategies encompassing enhanced surveillance, vector control, and preventive measures. Within this framework, ophthalmologists play a pivotal role in the early detection of infectious disease–related ocular signs, particularly during outbreaks of emerging arboviruses. Advances in vaccine development against Oropouche virus may have substantial public health benefits in endemic regions and may also contribute to broader progress in arboviral vaccine research.
REFERENCES
1. Olival KJ, Hosseini PR, Zambrana-Torrelio C, Ross N, Bogich TL, Daszak P. Host and viral traits predict zoonotic spillover from mammals. Nature. 2017 Jun 29;546(7660):646-650. Erratum in: Nature. 2017 Aug 31;548(7669):612.
2. Mohapatra RK, Mishra S, Satapathy P, Kandi V, Tuglo LS. Surging Oropouche virus (OROV) cases in the Americas: A public health challenge. New Microbes New Infect. 2024 Mar 26:59:101243.
3. Vasconcelos PF, Calisher CH. Emergence of Human Arboviral Diseases in the Americas, 2000-2016. Vector Borne Zoonotic Dis. 2016;16(5):295-301.
4. Zhang Y, Liu X, Wu Z, Feng S, Lu K, Zhu W, et al. Oropouche vírus: a neglected global arboviral threat. Virus Res. 2024 Mar:341:199318.
5. Sakkas H, Bozidis P, Franks A, Papadopoulou C. Oropouche fever: a review. Viruses. 2018;10(4):175.
6. Romero-Alvarez D, Escobar LE. Oropouche fever, an emergent disease from the Americas. Microbes Infect. 2018;20(3):135-146.
7. Bastos MS, Figueiredo LTM, Naveca FG, Monte RL, Lessa N, Figueiredo RMP, et al. Identification of Oropouche Orthobunyavirus in the cerebrospinal fluid of three patients in the Amazonas, Brazil. Am J Trop Med Hyg. 2012;86(4):732-5.
8. Ribeiro BFR, Barreto ARF, Pessoa A, Azevedo RDSS, Rodrigues FF, Borges BCB, et al. Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome. Viruses. 2025;17(3):397.
9. Lumsden WH. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952-53. II. General description and epidemiology. Trans R Soc Trop Med Hyg. 1955;49(1):33-57.
10. Manesh G, Giridhar A, Shebdele A, Kumar R, Saikumar SJ. A case of bilateral presumed chikungunya neuroretinitis. Indian J Ophthalmol. 2009;57(2):148–50.
11. Stanaway JD, Shepard DS, Undurraga EA, Halasa YA, Coffeng LE, Brady OJ, et al. The global burden of dengue: an analysis from the Global Burden of Disease Study 2013. Lancet Infect Dis. 2016;16(6):712-723.
12. Laude A, Chlebicki MP, Ang B, Barkham T. Maculopathy and dengue. Emerg Infect Dis. 2007;13(2):347-8.
13. Dick GW, Kitchen SF, Haddow AJ. Zika virus: Isolation and serological specificity. Trans R Soc Trop Med Hyg. 1952:46(5):509–20.
14. Miranda-Filho DB, Martelli CMT, Ximenes RAA, Araújo TVB, Rocha MAW, Ramos RCF, et al. Initial Description of the Presumed Congenital Zika Syndrome. Am J Public Health. 2016; 106(4):598-600.
15. Ventura CV, Ventura LO. Ophthalmologic Manifestations Associated With Zika Virus Infection. Pediatrics. 2018;141(Suppl 2):S161-S166.
16. 16. Khairallah M, Jelliti B, Jenzeri S. Emergent infectious uveitis. Middle East Afr J Ophthalmol. 2009;16(4):225-38.
17. Ganjian N, Riviere-Cinnamond A. Mayaro virus in Latin American and the Caribbean. Rev Panam Salud Publica. 2020 Feb 11:44:e14.
18. Benhar I, London A, Schwartz M. The privileged immunity of immune privileged organs: the case of the eye. Front Immunol. 2012 Sep 21;3:296.
| AUTHORS INFORMATIONS |
|
 |
» Diogo Gonçalves dos Santos Martins https://orcid.org/0000-0002-6881-5359 http://lattes.cnpq.br/2732051271384043 |
 |
» Paulo Schor https://orcid.org/0000-0002-3999-4706 http://lattes.cnpq.br/3542867700396961 |
 |
» Eduardo Damasceno https://orcid.org/0000-0002-7881-3584 http://lattes.cnpq.br/5017838124303708 |
 |
» Thiago Gonçalves dos Santos Martins https://orcid.org/0000-0002-3878-8564 http://lattes.cnpq.br/7906327075872528 |
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
January 22, 2025.
Accepted on:
February 5, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket