

Fábio Petersen Saraiva1; Milton Ruiz Alves2; Murilo Barreto Souza3; Patricia Grativol Costa Saraiva1; Luiz Guilherme Marchesi Mello1,2,4
DOI: 10.17545/eOftalmo/2026.0004
ABSTRACT
Refractometry is an essential procedure in ophthalmology for diagnosing refractive errors and associated diseases. A well-performed refraction examination improves visual function, reduces problems related to the adaptation of optical devices, and contributes to patients’ ocular health and well-being. In the current literature, there is a scarcity of publications providing guidelines for the steps of a refraction examination. With the aim of proposing a detailed protocol for this examination, a non-systematic literature review of scientific articles, procedural manuals on refraction techniques, and textbooks on ocular refractometry was conducted. The protocol presented herein includes guidance on equipment preparation, patient positioning, and the use of eye drops, as well as objective and subjective refraction techniques. The aim of the protocol is to minimize diagnostic variability, improve result accuracy, and provide support for both clinical practice and scientific research. Despite its systematization, the protocol emphasizes the importance of medical autonomy, as well as continuous training for ophthalmologists.
Keywords: Refractive errors; Guide; Ophthalmology; Ocular refraction; Refractometry.
RESUMO
A refratometria ocular é um procedimento essencial na Oftalmologia para diagnosticar erros refrativos e doenças associadas. O exame de refração bem executado melhora a função visual, reduz problemas relacionados à adaptação de recursos ópticos e contribui para a saúde ocular e o bem-estar dos pacientes. Na literatura atual, há escassez de informações com orientações quanto às etapas para realização do exame de refração. Com o objetivo de propor um protocolo detalhado para a execução deste exame, foi realizada uma revisão da literatura não sistemática em que foram revisados artigos, manuais de procedimentos sobre técnicas de refração e livros textos sobre a refratometria ocular. O protocolo apresentado inclui orientações sobre a preparação do ambiente, posicionamento do paciente, uso de colírios e métodos objetivos e subjetivos de refração. A proposta visa minimizar variabilidades diagnósticas, melhorar a acurácia dos resultados e oferecer suporte tanto para a prática clínica quanto para a pesquisa científica. Apesar de sua sistematização, o protocolo enfatiza a importância da autonomia médica, além do treinamento contínuo para oftalmologistas.
Palavras-chave: Erros de refração; Guia; Oftalmologia; Refração ocular; Refratometria.
INTRODUCTION
Refractometry is a technique used to determine the refractive errors of a patient’s eyes. It can be used to diagnose refractive errors and associated diseases1. The main objective of refractometry is to identify a patient’s refractive error and correct it through the prescription of optical aids, with the aim of treating ophthalmic conditions and providing comfort and improved vision. Uncorrected refractive error is the most common cause of low vision worldwide and is the main reason patients seek ophthalmic care2,3. Therefore, undergoing a refractive examination is also an opportunity to prevent, diagnose, and treat various ocular diseases. Refractometry is thus one of the most important examinations in ophthalmology and the most frequently performed procedure in this specialty4.
There are several methods for diagnosing refractive error. Regardless of the technique used, the measurement of refraction is not exact because of possible variations in parameters such as depth of field, pupil size, working distance, vertex distance, accommodation, and others. The greater the ametropia, the higher the level of uncertainty in the result, with variation ranging between ±0.25 and ±0.50 diopters (D)5. Therefore, it is essential to develop techniques that increase the success of refractometry and promote standardization in research.
Dissatisfaction with prescription eyeglasses is one of the main causes of lawsuits related to ophthalmology in Brazil6. Random or systematic errors in refractometry that lead to unreliable or invalid data can be minimized through the use of standardized protocols combined with adequate training programs7. Despite standardization and emphasis on training, substantial variability in measurements persists. This variability occurs not only in examinations performed by physicians during training but also in those conducted by experienced ophthalmologists. Therefore, efforts to reduce diagnostic variability should include continuous training, detailed refractometry protocols, and increased objectivity in the measurement of optical aberrations8.
An accurate refractive examination not only improves visual function but also reduces the frequency of problems related to poor adaptation to new eyeglasses or other optical aids, provides more reliable data for recording and analysis in scientific studies, and allows proper characterization and treatment of ophthalmic diseases. Thus, the aim of this article is to present a proposed sequence of steps for performing refractometry, thereby contributing to patients’ ocular health and well-being and promoting good clinical and research practices. This article does not intend to provide a detailed theoretical discussion of lenses, ocular physiology, or diseases, nor to define medical acts, including the prescription of optical aids. It should be noted that other techniques for performing refractometry exist. With respect for medical autonomy, this protocol does not dictate how the examination must be performed but rather represents a standardized refractometry approach that, when followed, can improve patient care by reducing errors and facilitate the standardization of techniques used in research.
METHODS
This study consists of a non-systematic literature review of scientific articles, procedural manuals on refraction techniques, and textbooks on refractometry, including guidelines published by ophthalmology societies and professional associations in Brazil. The keywords used to search the PubMed and Google Scholar databases were “ocular refraction,” “refractometry,” “ocular refractometry,” “eye refractometry,” “diagnostic techniques, ophthalmological,” and “physical examination,” in both English and Portuguese. Based on the data obtained, an operational protocol for performing refractometry was developed.
RESULTS
In the reviewed literature, there was a scarcity of data describing the sequence of steps for performing refractometry, even in textbooks on the subject. After analyzing the collected information, a step-by-step protocol for refractive examination was developed4,9-14:
Considerations before starting the examination
a. Room dimensions
The distance between the patient’s eyes and the visual acuity (VA) chart depends on the chart used. The Snellen chart should be placed at 6 m to assess distance vision, whereas the Jaeger chart should be positioned at approximately 40 cm to assess near vision. However, these distances must follow the specifications provided by the chart type and manufacturer.
b. Room lighting
Self-illuminated VA charts require a darkened room. Otherwise, the examination room should be adequately lit, in accordance with the lighting parameters recommended by the manufacturer.
c. Patient positioning
The patient should preferably be seated, with the eyes positioned at the same height as the VA chart.
d. Use of eye drops before the examination
Ideally, no eye drops with mydriatic or cycloplegic effects should be used before the examination begins.
e. Anamnesis
The patient’s chief complaint, history of the present illness, past medical and ocular history, and family history should be obtained. Certain clinical conditions can temporarily interfere with refraction, such as hypo- or hyperglycemia, pregnancy, and progressive cataracts. In such cases, the examination may be performed, but the prescription should be postponed until the clinical condition has stabilized. If the prescription of optical aids is indicated, the patient should be informed that refractive values may change with the resolution of the underlying condition.
f. Ocular examination
Refractometry should always be accompanied by a complete ophthalmologic examination to determine the most appropriate medical management for each patient. Complementary tests may be performed on an individual basis.
2. Objective dynamic refraction
At this stage, the examiner objectively determines the refractive error of the eye without cycloplegia. This can be performed using retinoscopy or autorefraction. It should be noted that high ametropia may not produce a retinoscopic reflex (“band”). If the reflex is not identified, retinoscopy should initially be performed using high plus and/or minus lenses in an attempt to visualize it. Once identified, the examination should proceed to item 3.
3. Subjective dynamic refraction
At this stage, the examiner determines the refractive error of one eye using information provided by the patient, based on the presentation of different lenses (spherical and/or cylindrical), without the use of cycloplegic agents. Subjective examination requires patient cooperation; when this is not possible, such as in young children or individuals with cognitive impairment, objective methods should be used to perform both dynamic (item 2) and static (item 4) refraction. The following steps should be performed for each eye individually:
3.1 After measuring VA, the refractive error identified during retinoscopy, autorefraction, or lensometry should be entered into the Greens refractor (phoropter) or a trial frame. Objective refraction is recommended as the initial step; however, if this is not feasible, the examination may begin with plano lenses. The Greens refractor or trial frame should then be centrally aligned with the patient’s eye, with the level and position checked relative to the visual axis of each eye. The vertex distance should be adjusted appropriately.
3.2 One eye should be occluded without exerting pressure. For standardization, it is suggested to initially occlude the left eye (OS).
3.3 Measure the VA of the examined eye.
3.4 Identify the line containing the smallest optotypes that the patient can correctly identify.
3.5 Test the spherical power to achieve the best possible vision
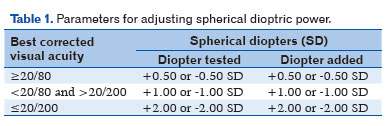
3.5.1 It is suggested to begin by offering a higher plus spherical diopter (DS) lens according to VA (Table 1) and asking the patient a question such as: “Does this lens make the letters sharper, blurrier, or is there no difference?”
3.5.1.1 If the response is “sharper” or “no difference,” continue adding plus DS lenses until the patient reports worsened vision. At that point, retain the previous lens and proceed to cylindrical power assessment (item 3.6).
3.5.1.2 If the response is “blurrier,” proceed to step 3.5.2.
3.5.2 Offer a minus lens according to Table 1 and ask a similar question: “Does this lens make the letters sharper, blurrier, or is there no difference?”
3.5.2.1 If the response is “sharper” and the patient is able to read additional optotypes, continue adding minus spherical lenses until the response becomes “no difference” or “blurrier.” The lens with the lowest minus power that provides the best VA should be selected. If the patient reports “sharper” vision but is unable to read more optotypes than previously, additional minus lenses should not be added. After identifying the least negative lens (closest to plano) that yields the best VA, proceed to cylindrical power assessment (item 3.6).
Note: During the examination, if the patient’s VA improves, spherical power should be reassessed using lenses corresponding to the newly achieved VA category (see Table 1).
3.6 Testing cylindrical dioptric power
If no cylindrical diopter (DC) is identified during objective refraction (retinoscopy, autorefractometry, or lensometry), or if objective refraction cannot be obtained, proceed to item 3.6.1. If DC is identified during objective refraction, proceed to item 3.6.2.
3.6.1 Place a cylindrical diopter at the 180° axis according to the patient’s VA (VA ≥ 20/80: −0.50 DC; VA <20/80 and ≥20/200: −1.00 DC; VA <20/200: −2.00 DC), and ask whether vision improves.
3.6.1.1 If VA improves with the addition of DC at the 180° axis, continue increasing the cylindrical power until VA no longer improves, and then proceed to refine the cylindrical axis (item 3.7). The spherical equivalent (SE) must be maintained during this stage of the examination. Example: Each time −0.50 DC is added, the SE must be maintained by adding +0.25 diopters sphere (SPH) to the total power. Thus, if a patient has a refraction of +0.50 SPH −0.50 DC at 180° and reports improved VA after the addition of −0.50 DC at 180°, and the DC is increased to −1.00 DC at 180° to maintain the SE, +0.25 SPH should be added, resulting in a final refraction of +0.75 SPH −1.00 DC at 180°.
3.6.1.2 If VA does not improve with the addition of DC at the 180° axis, repeat this step at the 45°, 90°, and 135° axes. If VA improves at any of these axes, continue increasing the cylindrical power until VA no longer improves, and then proceed to refine the cylindrical axis (item 3.7). However, if VA does not improve at any of these axes, do not add DC and proceed to refine the spherical power (item 3.9).
3.6.2 If DC is identified during objective refraction, ask the patient to fixate on the smallest line they can discern on the VA chart and test the cylindrical power. If VA is ≥ 20/80, add ±0.50 DC and ask: “Is the first lens or the second lens better?” In this question, the first lens corresponds to the initial diopter, whereas the second lens corresponds to the new diopter presented with the addition of ±0.50 DC. For VA worse than 20/80, use ±1.00 DC for the tests described above.
3.6.2.1 If the patient reports being unable to perceive a difference between the two lenses presented, remove 0.50 DC from the Greens refractor or trial frame and repeat item 3.6.2 until the patient can perceive a difference (proceed to item 3.6.2.2 if the first lens is preferred or to item 3.6.2.3 if the second lens is preferred), or until zero cylindrical power is reached. If zero DC is reached, proceed to refine the spherical power (item 3.9).
3.6.2.2 If the patient reports worsening VA after the addition or removal of DC, reverse the initial action. Example: If adding −0.50 DC results in worsened VA, remove −0.50 DC. If both the addition and removal of the same cylindrical power have been attempted and the patient continues to prefer the first lens—that is, VA worsens with both changes—proceed to refine the cylindrical axis (item 3.7).
3.6.2.3 If the patient prefers the addition of DC (plus or minus), that is, if the second lens is judged better, retain the new cylindrical power and maintain the previous SE by adding half of the cylindrical power change to the spherical component. Repeat the comparison described in item 3.6.2 until the patient prefers the first lens, and then proceed to refine the cylindrical axis (item 3.7).
3.7 Testing the cylindrical axis
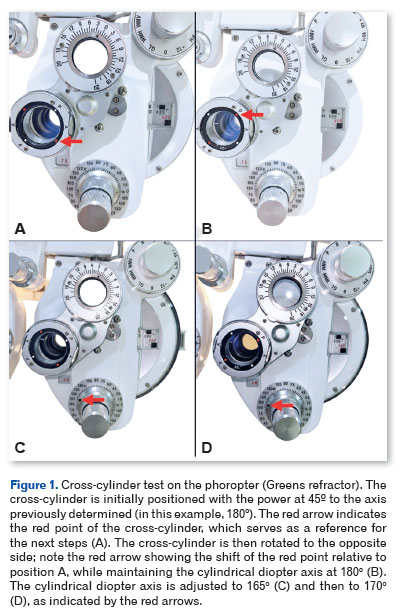
After determining the cylindrical power, it is necessary to refine the cylindrical axis. If the patient’s VA is ≤ 20/200, the use of a ±1.00 DC Jackson cross-cylinder is recommended. To perform this step, the patient should fixate on optotypes located two lines above the smallest line identified on the VA chart, ensuring that the optotypes can be clearly recognized (e.g., if the smallest readable line is 20/30, the patient should be instructed to look at the 20/50 line). The patient should be guided to focus on a letter with rounded contours. Next, the examiner should position the cross-cylinder so that its axis is oriented at 45° relative to the previously determined cylindrical axis (obtained by objective refraction or item 3.6.1) and inform the patient that vision may become slightly blurrier during this test. The cross-cylinder test should then be performed by alternately flipping the lens (Figure 1A and B), while asking a question such as: “Which lens is better: the first, the second, or are both lenses similar?”
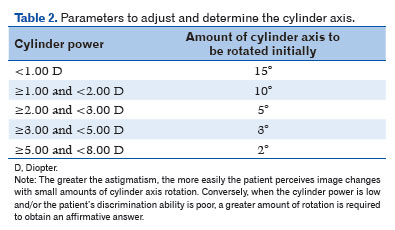
3.7.1 If the patient prefers one position of the cross-cylinder over the other (e.g., the first lens over the second), and a minus-cylinder phoropter is being used (as is most common in Brazil), the axis of the cylindrical lens should be rotated toward the negative axis of the cross-cylinder (indicated by the red dot on the phoropter), according to the adjustment suggested in Table 2. Item 3.7 should then be repeated until the patient reports that both lenses are similar, progressively reducing the angular range of rotation when reversing the direction of rotation. Example: If a patient with −0.75 DC at 180° initially prefers the lens corresponding to a clockwise rotation of the cross-cylinder (Figure 1A), the cylindrical axis should be rotated 15° clockwise, resulting in −0.75 DC at 165° (Figure 1C). If, during the subsequent cross-cylinder test with −0.75 DC at 165°, the patient prefers the lens corresponding to counterclockwise rotation (Figure 1B), the cylinder should be rotated 5° counterclockwise, yielding −0.75 DC at 170° (Figure 1D). This process should continue until the patient reports that both lenses are similar. The correct axis corresponds to the position at which both lenses are perceived as similar.
3.7.2 If the patient reports that both lenses are similar and this is the first cross-cylinder test performed in that eye, rotate the cylindrical axis 15° clockwise or counterclockwise and repeat item 3.7 to confirm that the axis is correctly positioned.
3.7.3 If the patient reports that both lenses are similar and this is not the first cross-cylinder test in that eye, the cylindrical axis refinement is complete, and the examiner should proceed to refine the cylindrical power (item 3.8).
3.8 Refining the cylindrical power
For refinement of cylindrical power, the patient must have VA ≥20/400. If VA is worse than 20/400, proceed directly to refinement of the spherical power (item 3.9).
3.8.1 Ask the patient to fixate on the smallest line they can discern on the VA chart. It is suggested to begin by adding ±0.25 DC in cases of VA ≥20/80 and ±0.50 DC in cases of VA <20/80 and ≥20/400. At the same time, ask a question such as: “Is the first lens or the second lens better?” In this context, the first lens corresponds to the initial cylindrical power, whereas the second lens corresponds to the new cylindrical power presented with the addition of ±0.25 DC or ±0.50 DC.
3.8.1.1 If the patient perceives no difference between the two lenses, select the lens with the cylindrical power closest to zero and repeat the procedure described in item 3.8.1 until a difference is perceived (proceed to item 3.8.1.2 if the first lens is preferred or to item 3.8.1.3 if the second lens is preferred), or until zero cylindrical power is reached. If zero DC is reached, proceed to refine the spherical power (item 3.9).
3.8.1.2 If the patient prefers the first lens, indicating worsened VA after the addition or removal of DC (the second lens), reverse the initial action. Example: If, after adding −0.50 DC, the patient prefers the first lens (prior to the addition), repeat the comparison described in item 3.8.1 after removing −0.50 DC. If both addition and removal of the same cylindrical power have been attempted and the patient continues to prefer the first lens, proceed to refine the spherical power (item 3.9).
3.8.1.3 If the patient prefers the addition of DC (plus or minus), that is, if the second lens is judged better, retain the new cylindrical power and maintain the previous SE by adding half of the cylindrical power change to the spherical component. Repeat the comparison described in item 3.8.1 until the patient prefers the first lens, and then proceed to refine the spherical power (item 3.9).
3.9 Refining spherical dioptric power
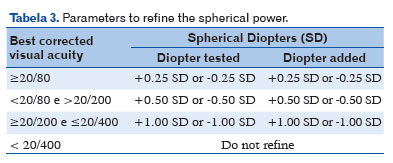
At this stage, the patient should be instructed to fixate on the line containing the smallest optotypes they can accurately identify. It is suggested to begin by adding plus DS according to VA (Table 3) and asking a question such as: “Does this lens make the letters sharper, blurrier, or is there no difference?”
3.9.1 If the response is “sharper” or “no difference,” continue adding plus DS until the patient reports that vision has become “blurrier.” At that point, select the previous diopter and proceed to item 3.9.3.
3.9.2 If the response is “blurrier,” retain the previous DS and repeat the question described in item 3.9; however, instead of adding plus DS, add minus DS. If the response is “sharper” and the patient is able to read additional optotypes with the new diopter, continue repeating step 3.9.2 until the response becomes “no difference” or “blurrier,” and then proceed to item 3.9.3. If the patient reports “sharper” vision but is unable to read more optotypes with the new diopter, proceed directly to item 3.9.3.
3.9.3 After determining the refractive error, the binocular balance of accommodation test is performed in patients with accommodative capacity in both eyes (it is not performed, for example, in cases of pseudophakia or monocular vision) to ensure that the level of accommodation is balanced between the two eyes (OU). This test is performed only when VA is relatively similar in OU. We suggest performing the balance test using plus lenses and prisms. In this procedure, both eyes are kept unoccluded. Plus lenses of +0.75 DS are added in OU to relax accommodation, and vertical prisms (Risley prisms in the phoropter) are used to dissociate the images of the two eyes—usually 3 prism diopters base up in the right eye (OD) and 3 prism diopters base down in the OS. The patient’s vision may then be somewhat blurred, and they should be presented with optotypes two lines above the smallest line they were initially able to see. For example, in a patient with corrected VA of 20/20 in OU, the 20/30 optotype line should be presented after adding the plus lenses and prisms for the binocular balance test. This line will be perceived as two separate lines: a lower line seen by the OD and an upper line seen by the OS. The patient is then asked whether the optotypes in the two lines are equally sharp, equally blurred, or sharper in one line than in the other. If the optotypes in the upper line (OS) are clearer, +0.25 DS is added to the OS. The question is repeated, and if the upper line remains clearer, an additional +0.25 DS is added to the OS. Conversely, if the optotypes in the lower line (OD) are clearer, +0.25 DS is added to the OD and the question is repeated. When the patient reports that the optotypes in both lines are equally sharp or equally blurred, the prisms and the initial +0.75 DS overcorrection added to relax accommodation are removed.
3.10 Evaluating refractive error for near vision (near addition)
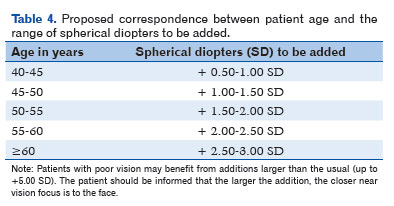
This stage is performed in preterm infants, in eyes that have undergone facetectomy, and in other situations deemed appropriate by the ophthalmologist. If the patient does not meet these criteria, you should proceed directly to the static refraction assessment (item 4). Measurement of refractive error to improve near VA may be performed binocularly (OU) without occlusion or monocularly in each eye, depending on the ophthalmologist’s judgment. The patient’s ability to focus at near distance (35–40 cm) should be assessed by adding the minimum amount of plus lens power required to achieve the best possible near VA using a near vision chart. We suggest using the Jaeger chart at this stage. Table 4 provides suggested ranges of plus DS additions according to age group. In eyes that have undergone facetectomy, a near addition of +2.50 to +3.00 DS should be considered. For other accommodative disorders, the ophthalmologist should determine the appropriate dioptric addition based on recommendations in the literature. It should be noted that accommodative capacity (amplitude of accommodation [AA]) may differ between the two eyes. A simple method for measuring accommodative capacity is to ask the patient to read the second line of the Jaeger reading card (J2) while wearing the determined distance correction. The card is slowly moved toward the eye until the patient reports blurring of the optotypes. When a slight blur is first noticed, the card is moved closer to confirm that the blur worsens, and then moved away until the image becomes clear again. The distance between the card and the corrective lens worn by the patient is then measured. The AA is calculated using the formula: AA (in diopters) = 1 / distance from the card to the lens (in meters) For example, if blurring occurs at a distance of 10 cm, the AA is 1 / 0.1, or 10 diopters.
After completing this stage, proceed to the static refraction assessment (item 4).
4. Static refraction
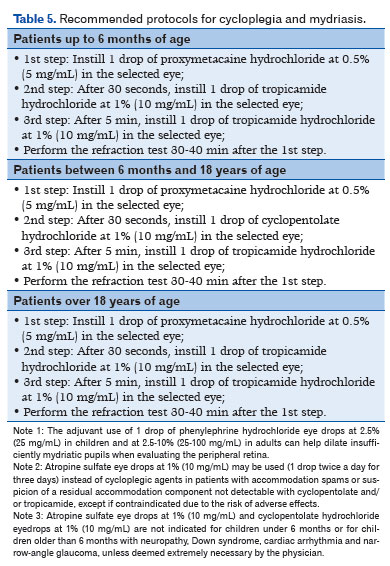
This stage requires the use of cycloplegic eye drops, followed by an appropriate waiting period for their effect. The patient and/or guardian should be informed about possible side effects. It is important to compress the lacrimal sac immediately after instillation of the eye drops to reduce the risk of systemic absorption and to increase the ocular contact time of the medication, especially in children and in adults with comorbidities. Given the need to use pharmacological agents during the refractive examination, this procedure should always be supervised by an ophthalmologist. It should be noted that, depending on the individual patient’s clinical characteristics and diagnostic considerations, the use of alternative cycloplegic and mydriatic eye drops may be necessary, at the ophthalmologist’s discretion. For cycloplegia, the use of eye drops as described in Table 5 is recommended4,9,15-17.
4.1 Objective static refraction
In cases where subjective methods are difficult or unreliable, objective methods should be used to determine the patient’s refractive error, either through retinoscopy (preferred) or an autorefractor. If the patient is able to provide adequate feedback regarding optotypes, subjective static refraction (item 4.2) should be prioritized.
4.2 Subjective static refraction
If the patient is under 40 years of age, or over 40 and suspected of accommodating during dynamic refraction (e.g., patients requiring more than the expected near addition for their age group - Table 4), it is mandatory to perform a static refraction assessment following dynamic refraction.
At this stage, only the spherical power for distance should be refined, with each eye examined separately. Plus spherical lenses should be added to the power determined during dynamic refraction, and the patient should be asked whether VA improves, worsens, or remains unchanged. Additional plus lenses should be added as long as the patient reports either improved VA or no difference between the lenses presented. If the patient reports worsening VA with the added plus lens, the assessment for that eye should be terminated, and the contralateral eye should then be examined. If the accommodation reflex interfered with the dynamic refraction, the final spherical value obtained in the static refraction is expected to be more positive.
During cycloplegia, the pupil may dilate to 6–9 mm, exposing part of the peripheral cornea and lens, whose refractive power differs from the central zone. This dilation can lead to changes in the axis and power of astigmatism. For this reason, cylindrical power and axis should not be tested or modified during the static refraction evaluation.
DISCUSSION
Refraction is a fundamental clinical measurement in eye examination. Ametropia is not only the condition that most frequently prompts patients to seek ophthalmic care, but the data obtained from refractometry, when properly performed and interpreted, also provide a basis for guiding medical management in the treatment of various ocular diseases and in the promotion of eye health2-4. There are multiple methods for assessing an eye’s refractive error, which can result in variability in refractometry data, potential errors in clinical analysis, and increased bias in research studies.
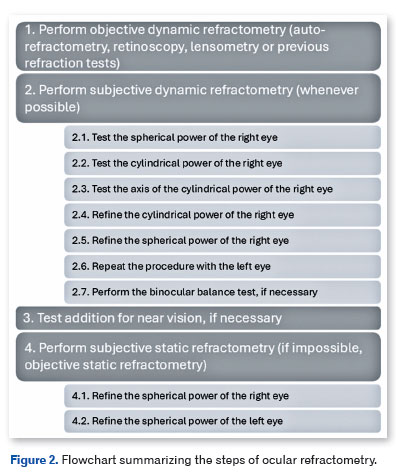
We did not find any detailed systematization of refractometry in the literature. Although systematization may seem to imply limitations on clinical practice, this article does not aim to prescribe exactly how refractometry should be performed; rather, it proposes a structured workflow for conducting the examination (Figure 2). Ophthalmologists may choose to perform additional tests or modify the steps as clinically indicated.
Over the years, various types of equipment have been developed to improve refractometry. However, to date, no device has proven superior to the assessment performed by an experienced ophthalmologist18,19, nor can such equipment interpret the data obtained or determine the optimal management for a specific patient. Moreover, ametropias are closely associated with structural alterations of the eye and with diseases that can cause potentially irreversible damage to vision, overall health, and quality of life20-23. For refractometry to maintain its clinical value, it must be performed by physicians trained in ophthalmology. Ophthalmology training centers should provide continuous education in refractometry, and standardization of examination steps should be maintained while respecting the particularities of each patient.
This study proposes a sequence of steps that, if followed correctly, can accurately determine a patient’s ametropia to guide clinical decisions. Additionally, it aims to facilitate the training of ophthalmology residents, assist practicing ophthalmologists in daily clinical work, serve as a model for standardizing refractometry in medical institutions and research, and reinforce the importance of having refractive examinations performed by trained doctors to improve population eye health.
REFERENCES
1. Bicas HE, Gonçalves ER. Refratometria ou Optometria?: SciELO Brasil; 2004. p. 853-4.
2. Jeganathan VSE, Robin AL, Woodward MA. Refractive error in underserved adults: causes and potential solutions. Curr Opin Ophthalmol. 2017;28(4):299-304.
3. Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86(1):63-70.
4. Alves MR, Polati M, Julio S. Refratometria ocular e a arte da prescrição médica. Rio de Janeiro: Cultura Médica; 2017.
5. Smith G. Refraction and visual acuity measurements: what are their measurement uncertainties? Clinical and Experimental Optometry. 2006;89(2):66-72.
6. Santos W, Solari HP, Ventura MP. Processos judiciais em oftalmologia: análise de possíveis fatores desencadeantes. Arq Bras Oftalmol. 2010;73(6):501-4.
7. Klein R, Klein BE, Moss SE, DeMets D. Inter-observer variation in refraction and visual acuity measurement using a standardized protocol. Ophthalmology. 1983;90(11):1357-9.
8. Kahn HA, Leibowitz H, Ganley JP, Kini M, Colton T, Nickerson R, et al. Randomized controlled clinical trial. National Eye Institute workshop for ophthalmologists. Standardizing diagnostic procedures. Am J Ophthalmol. 1975;79(5):768-75.
9. Alves AdA. Cultura Médica. 2014.
10. Terheyden JH, Holz FG, Schmitz-Valckenberg S, Lüning A, Schmid M, Rubin GS, et al. Clinical study protocol for a low-interventional study in intermediate age-related macular degeneration developing novel clinical endpoints for interventional clinical trials with a regulatory and patient access intention—MACUSTAR. Trials. 2020;21:1-11.
11. Early Treatment Diabetic Retinopathy Study Research Group (ETDRS). Manual of Operations. Baltimore: ETDRS Coordinating Center, University of Maryland. Available from: National Technical Information Service, 5285 Port Royal Road, Springfield, VA 22161; Accession No. PB85 223006/AS.
12. Hofmeister EM, Cason JB, Murdoch DM, Yau IW, Wang Y, Parizadeh DD, et al. Wavefront-guided PRK treatment of myopia using a refractive aberrometer. J Cataract Refract Surg. 2023;49(3):292-8.
13. Bicas HE, Alves AdA, Uras R. Refratometria ocular. Refratometria ocular. 2005. p. 400.
14. Alvez M, Bicas H. Refratometria ocular e visão subnormal. Conselho Brasileiro de Oftalmologia. 2018.
15. Curi I, Nakayama SA, Pereira EM, Hopker LM, Ejzenbaum F, Barcellos RB, et al. Brazilian guideline for pediatric cycloplegia and mydriasis. Arq Bras Oftalmol. 2023;86(4):388-96.
16. Levine L. Effective degree of mydriasis with phenylephrine and tropicamide. Am J Optom Physiol Opt. 1976;53(12):774-85.
17. Diamond JP. Systemic adverse effects of topical ophthalmic agents. Implications for older patients. Drugs Aging. 1997; 11(5):352-60.
18. Rao DP, Negiloni K, Gurunathan S, Velkumar S, Sivaraman A, Baig AU, et al. Validation of a Simple-to-Use, Affordable, Portable Wavefront Aberrometry-Based Auto Refractometer in a Paediatric Population. Clin Ophthalmol. 2022;16:4281-91.
19. Rao DP, Negiloni K, Gurunathan S, Velkumar S, Sivaraman A, Baig AU, et al. Validation of a simple-to-use, affordable, portable, wavefront aberrometry-based auto refractometer in the adult population: A prospective study. BMC Ophthalmol. 2022;22(1):498.
20. Verhoeven VJ, Wong KT, Buitendijk GH, Hofman A, Vingerling JR, Klaver CC. Visual consequences of refractive errors in the general population. Ophthalmology. 2015;122(1):101-9.
21. Abrahamsson M, Fabian G, Sjostrand J. Refraction changes in children developing convergent or divergent strabismus. Br J Ophthalmol. 1992;76(12):723-7.
22. Jacobson DM. Intracranial hypertension and the syndrome of acquired hyperopia with choroidal folds. J Neuroophthalmol. 1995;15(3):178-85.
23. Herbort CP, Papadia M, Neri P. Myopia and inflammation. J Ophthalmic Vis Res. 2011;6(4):270-83.
| INFORMAÇÕES DOS AUTORES |
|
 |
» Fábio Petersen Saraiva http://lattes.cnpq.br/4779368875052793 http://orcid.org/0000-0002-1196-8872 |
 |
» Milton Ruiz Alves http://lattes.cnpq.br/6210321951145266 http://orcid.org/0000-0001-6759-5289 |
 |
» Murilo Barreto Souza http://lattes.cnpq.br/8476124036191411 http://orcid.org/0000-0002-2965-2737 |
 |
» Patricia Grativol Costa Saraiva http://lattes.cnpq.br/8944400266170157 http://orcid.org/0000-0002-1083-9980 |
 |
» Luiz Guilherme Marchesi Mello http://lattes.cnpq.br/0620671396588526 http://orcid.org/0000-0001-8347-2393 |
Funding: The authors declare no funding.
Conflict of interest: The authors declare no conflicts of interest.
Received on:
February 24, 2025.
Accepted on:
December 6, 2025.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket