

André Augusto Homsi Jorge; Felipe de Andrade Budin; Livia Norcia Zenerato; Ana Laura Pallone Buzzini
DOI: 10.17545/eOftalmo/2024.0029
ABSTRACT
OBJECTIVE: To evaluate the relationship between optical correction and the progression of hyperopia in children.
METHODS: The medical records of patients were analyzed and divided into three groups according to the optical correction used and the spherical equivalent.
RESULTS: The mean annual decrease in hyperopia differed among the groups, without statistical significance.
CONCLUSION: There was no statistically significant relationship between the progression of hyperopia and optical correction.
Keywords: Hyperopia; Ophthalmology; Eyeglasses; Ocular refraction.
RESUMO
OBJETIVO: Avaliar a relação entre a correção óptica utilizada e a evolução da hipermetropia em crianças.
MÉTODOS: Análise de prontuários com separação em três grupos de acordo com a correção óptica utilizada e o equivalente esférico hipermetrópico.
RESULTADOS: Diminuição da hipermetropia média anual foi diferente entre os grupos, porém sem relevância estatística.
CONCLUSÃO: Sem relevância estatística entre a evolução da hipermetropia e a correção óptica utilizada.
Palavras-chave: Hipermetropia; Oftalmologia; Óculos; Refração ocular.
INTRODUCTION
Hyperopia is a refractive error in which light rays coming from infinity are brought into focus by the ocular optical system (in its relaxed accommodative state) behind the retina. Its etiology can be axial (small eyes), refractive (changes in curvature, as in the case of a flat cornea; changes in the refractive index, as in some types of cataracts; and aphakia), or mixed. Despite the apparent worldwide increase in myopia cases, hyperopia appears to be the most prevalent refractive error, particularly among children. In moderate to high levels, it is commonly associated with accommodative esotropia, and in very high levels, it can lead to bilateral refractive amblyopia1.
The changes in the axial diameter and in the curvature of the cornea and lens that occur in the first years of life determine refractive changes, a process known as emmetropization. The average axial diameter of a newborn’s eye is 17 mm, which by itself would cause hyperopia of approximately 21 diopters (D). However, this is offset by an increase in the curvature of the cornea (on average 51.2 D at birth) and of the lens. As the child grows, the eye lengthens by approximately 7 mm until adulthood, the cornea reduces its curvature (mainly in the first 6 months) to approximately 43 D, and the refractive power of the lens decreases by an average of 8 D during the first year of life. In a study conducted in Belo Horizonte by Ribeiro et al., children had an average hyperopia of 2.099 D in the first year of life, which increased to 3.424 D in the fourth year, followed by a slight reduction to 2.973 D in the fifth year, remaining without significant differences until the tenth year2.
This study aimed to analyze the progression of hyperopia in children and the influence of the magnitude of ametropia and optical correction.
METHODS
This was a retrospective cohort study based on an analysis of the medical records of patients with hyperopia who were followed at the Hospital Oftalmológico do Interior Paulista in Araraquara/SP, in the strabismus outpatient clinic. The medical records of patients monitored between 2015 and 2021 were collected and analyzed between April and June 2022. A total of 137 eyes of patients aged 3–5 years with hyperopia were selected, with or without an indication for optical correction for the presented ametropia. Based on the collected data, these eyes were classified into three groups, considering the spherical equivalent and the optical correction used. The eyes were assessed individually, and the same patient could belong to two different groups.
Group 1 consisted of 76 eyes with hyperopia in children aged 3–5 years, with a spherical equivalent of up to +3.25 D and no optical correction. Group 2 consisted of 33 eyes with hyperopia in children aged 3–5 years, with a spherical equivalent of +3.25 D and wearing partial optical correction. Group 3 consisted of 28 eyes with hyperopia in children aged 3–5 years, with a spherical equivalent of +3.25 D or more, with accommodative esotropia and wearing full optical correction. Under-correction in the study groups ranged from 1.0 to 1.50 D. Subsequently, the groups were analyzed when their participants were aged 9–11 years.
All measurements were obtained in a standardized manner, after cycloplegia with one drop of cyclopentolate and one drop of tropicamide (administered 5 minutes after cyclopentolate), using objective refraction with a Potec autorefractor (model PRK 8.000). Measurements were performed 40 minutes after tropicamide administration. Cycloplegia was always preceded by administering a drop of 0.5% proxymetacaine hydrochloride.
All eye examinations showed no abnormalities, with the exception of Group 3, which had accommodative esotropia.
The groups were compared using one-way analysis of variance. The Tukey Honestly Significant Difference (HSD) post hoc test was used to evaluate multiple comparisons when the result was significant. The effect sizes were interpreted using the following reference values: Generalized Eta Squared (η2) small (~0.01), medium (~0.06), and large (~0.14)3. All procedures were performed using R® software (version 4.3.1, R Core Team, Vienna, Austria).
This study was approved by the Ethics Committee of the Hospital Infantil Darcy Vargas under protocol number 58332022.0.0000.0167.
RESULTS
Table 1 shows the stratified data describing the profile of the study groups. We analyzed 85 eyes of female patients and 48 eyes of male patients. Group 1 included 47 eyes of female patients and 29 eyes of male patients. Group 2 included 21 eyes of female patients and 8 eyes of male patients. Group 3 included 17 eyes of female patients and 11 eyes of male patients. In total, 137 eyes were evaluated.
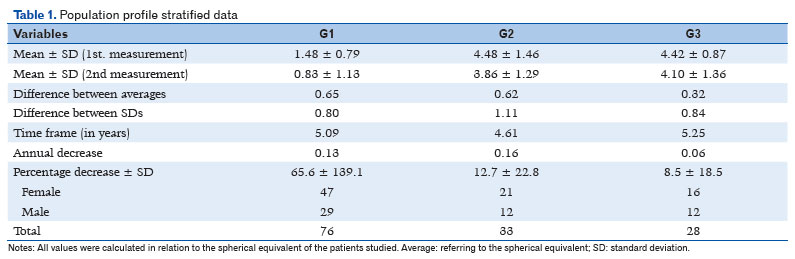
The average spherical equivalent values for Group 1 were 1.48 D at the first measurement and 0.83 D at the second measurement (a difference of 0.65 D). The standard deviation was 0.79 for the first measurement, 1.13 for the second measurement, and 0.80 for the difference between measurements. The average interval between measurements was 5.09 years.
The average spherical equivalent values for Group 2 were 4.48 D at the first measurement and 3.86 D at the second measurement (a difference of 0.62 D). The standard deviation was 1.46 for the first measurement, 1.29 for the second measurement, and 1.11 for the difference between measurements. The average interval between measurements was 4.61 years.
The average spherical equivalent values for Group 3 were 4.42 D at the first measurement and 4.10 D at the second measurement (a difference of 0.32 D). The standard deviation was 0.87 for the first measurement, 1.36 for the second measurement, and 0.84 for the difference between measurements. The average interval between measurements was 5.25 years.
The difference in the average time between measurements among the three groups was not statistically significant (p=0.1029). The average annual reductions were 0.13, 0.16, and 0.06 D in Groups 1, 2, and 3, respectively.
The percentage reductions in hyperopia were 65.6 ± 139.1, 12.7 ± 22.8, and 8.5 ± 18.5 in Groups 1, 2, and 3, respectively.
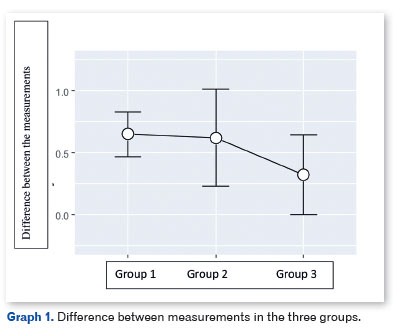
Graph 1 shows the differences between the two measurements in the three groups. There was no difference between the groups regarding the change between measurements 1 and 2 (F=1.46; p=0.24; η2=0.021).
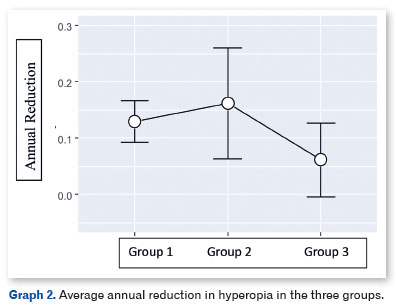
Graph 2 shows the average annual reduction in hyperopia in the three groups. There was no difference between the groups in terms of annual reduction in hyperopia (F=2.06; p=0.13; η2=0.030).
Graph 3 shows the percentage reduction in hyperopia in the three study groups. There was a significant difference between the groups in the percentage reduction in hyperopia (F=4.62; p=0.011; η2=0.065).
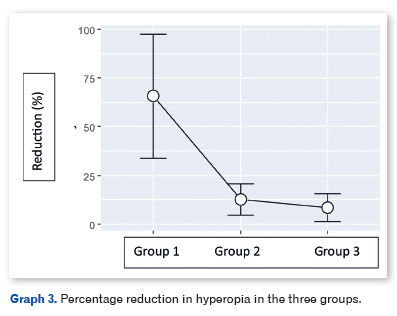
The Tukey HSD post hoc comparison showed significant differences between Groups 1 and 2 (p=0.0447) and between Groups 1 and 3 (p=0.0401). There was no difference between Groups 2 and 3 (p=0.99).
DISCUSSION
Several theories about the progression of hyperopia in children have been presented in the literature. Some authors support the idea that eye growth and emmetropization are directly correlated with the patient’s accommodation, which is influenced (either to a lesser or greater extent) by the optical correction prescribed. Accommodation results in a change in the shape of the lens, which becomes more curved to increase its dioptric power due to relaxation of the zonule that connects the lens to the ciliary body. This relaxation occurs through contraction of the ciliary muscle, which is innervated by the third cranial nerve and functions as an involuntary autonomic mechanism.
Therefore, some authors advocate that accommodation (which places the image on the retina) results in inhibiting the stimulus for axial growth toward the image formed behind the retina. In myopic eyes, there is no accommodation because the image is formed anterior to the retina, and axial growth tends to be greater than in hyperopic eyes, consistent with the theory that full accommodation slows axial growth4,5. Other authors propose that highly hypermetropic eyes (which are smaller, when the axial factor is considered) have thicker sclerae and are less susceptible to axial growth than larger eyes (with thinner sclerae)6. Previous studies have concluded that the greater the hyperopia, the less emmetropization occurs, with patients tending toward stability over the years7,8. Thus, conclusions can be drawn that support both theories described above, as high hyperopia is usually accompanied by accommodative esotropia, which requires full correction9. Accommodation activates visual convergence mechanisms, which explains the correlation between esotropia and the substantial accommodative demand caused by higher hyperopia8-10. Full correction could lead to reduced accommodation and, consequently, reduced stimulation of axial growth, according to the first theory. On the other hand, high hyperopia is also associated with a thicker sclera due to the smaller size of the eye (considering axial factors). As a result, lower rates of axial growth and smaller reductions in hyperopia would be expected.
There is considerable uncertainty about the effect of full correction of hyperopia on the emmetropization process, and there is no consensus in the literature on this topic. In a study published in 1984, Silva et al.10 found no significant change in hyperopia between the age groups of 0–2 and 4–6 years in both patients with and without strabismus. In that study, hyperopia began to decrease in non-strabismic individuals at around 5 years of age, ending at approximately 13 years. In strabismic individuals, this decrease began at around 7 years of age and continued until at least 18 years. However, Cunha et al.11, in a study published in 2017, concluded that the constant use of full optical correction for hyperopia inhibits the natural emmetropization process in cases of high hyperopia during childhood.
We evaluated a series of articles published between 2010 and 20194-9 and found that almost all authors concluded that there is a difference in the progression of hyperopia between strabismic and non-strabismic patients. However, there is no consensus regarding when this divergence occurs: some state that hyperopia decreases more in non-strabismic patients throughout childhood, whereas others argue that this only occurs in late childhood or adolescence. Another question that remains unresolved regarding the smaller reduction in hyperopia in patients with strabismus is whether this is due to the use of full correction (which results in less accommodative effort) or due to the fact that these eyes tend to have higher hyperopia and, consequently, smaller axial diameters and thicker, less distensible sclerae (which are more resistant to axial growth). Paradoxically, Park et al.8 concluded that larger degrees of hypermetropia showed greater reductions.
Our results showed that the pattern of hyperopia reduction between the ages of 3–5 and 9–11 years did not differ among the three groups studied; in other words, the reduction in hyperopia was not affected by the degree of ametropia or the amount of correction used. These conclusions can be drawn particularly from the comparison of Group 1 with Group 2 (the magnitude of hyperopia was not a determining factor in its reduction) and from that of Group 2 with Group 3 (the amount of optical correction was not a determining factor in the reduction). These results contradict the findings of most previous studies.
This study has some limitations. For instance, we did not evaluate corneal curvature or axial length, and the dispersion of the data in our sample was very large, which at times resulted in wide confidence intervals. Moreover, because this was a retrospective study, it was not possible to administer questionnaires to assess whether the children consistently wore their glasses.
In our study, the magnitude of hyperopia and the optical correction used did not influence the progression of ametropia in these children. We emphasize that the conclusions drawn here should be limited to the sample included in this study.
Further studies should be conducted to assess variations in corneal curvature and axial length in these situations.
REFERENCES
1. Ferraz FHS. Perfil de distribuição de erros refracionais no sul do centro-oeste do estado de São Paulo e seu impacto na acuidade visual: estudo de base populacional [tese]. São Paulo: Universidade Estadual Paulista, Faculdade de Medicina de Botucatu; 2013. Disponível em: http://hdl.handle.net/11449/105628.
2. Ribeiro GB, Gonçalves RM, Diniz CM, Paula ST, Almeida HC. Evolução da hipermetropia na infância. Arq Bras Oftalmol. 2004;66(1):83-6.
3. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York: Routledge; 1988. https://doi.org/ 10.4324/9780203771587
4. Yang HK, Choi JY, Kim DH, Hwang JM. Changes in refractive errors related to spectacle correction of hyperopia. PLoS One. 2014;9(11):e110663.
5. Ahn YJ, Park SH, Shin SY. Changes in axial length in accommodative esotropia patients with minimal hyperopic correction. PLoS One. 2019;14(1):e0203584.
6. Hu Y, Ding X, Zeng J, Cui D, Li C, He M, Yang X. Longitudinal changes in spherical equivalent of moderate to high hyperopia: 2- to 8-year follow-up of children at an initial age of 5.5 to 8.4 years. Invest Ophthalmol Vis Sci. 2019;60(8):3127-34.
7. Birch EE, Stager DR, Wang J, O’Connor A. Longitudinal changes in refractive error of children with infantile esotropia. Eye (Lond). 2010;24(12):1814-21.
8. Bonafede L, Bender L, Shaffer J, Ying GS, Binenbaum G. Refractive change in children with accommodative esotropia. Br J Ophthalmol. 2020;104(9):1283-7.
9. Park KA, Kim SA, Oh SY. Long-term changes in refractive error in patients with accommodative esotropia. Ophthalmology. 2010;117(11):2196-207.e1.
10. Silva MHA, Araújo JS, Souza-Dias CR. Evolução da hipermetropia na infância e adolescência. Arq Bras Oftalmol. 1984;47(4):146-53.
11. Cunha CM, Correia RJB e Cunha JT. Correção óptica e evolução da hipermetropia. Rev Bras Oftalmol. 2017;76(4):194-7.
| AUTHORS INFORMATIONS |
|
 |
»André Augusto Homsi Jorge https://orcid.org/0000-0001-6973-7172 http://lattes.cnpq.br/6689964323533092 |
 |
» Felipe de Andrade Budin https://orcid.org/0009-0002-1958-2576 http://lattes.cnpq.br/6330057023786152 |
 |
» Livia Norcia Zenerato |
 |
» Ana Laura Pallone Buzzini https://orcid.org/0009-0009-3399-6311 http://lattes.cnpq.br/2476172101360567 |
Funding: The authors declare no funding.
Ethics committee approval: Hospital Infantil Darcy Vargas (CAAE: 58332022.0.0000.0167).
Conflicts of interest: The authors declare no conflicts of interest.
Received on:
August 15, 2024.
Accepted on:
November 26, 2024.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket