

Luciana da Cruz Noia1,2
DOI: 10.17545/eOftalmo/2023.0045
Este artigo pertence à Edição Especial Neuroftalmologia por imagem: acima e além
A 61-year-old man with a history of sudden and painless lower visual field defected for approximately 7-8 months.
General systemic complaints: the patient denied nausea, vomiting, or alterations in strength, sensitivity, or speech.
The patient denied any previous history of ophthalmic diseases.
Personal history: systemic arterial hypertension, diabetes mellitus.
On examination
Visual acuity: 20/20 in both eyes (OU).
Pupillary reflexes present and symmetrical, with no relative afferent pupillary defect.
External ocular muscles: no changes.
Intraocular pressure: 14mmHg in OU.
Biomicroscopy without changes.
Fundus: no changes.
Complementary tests
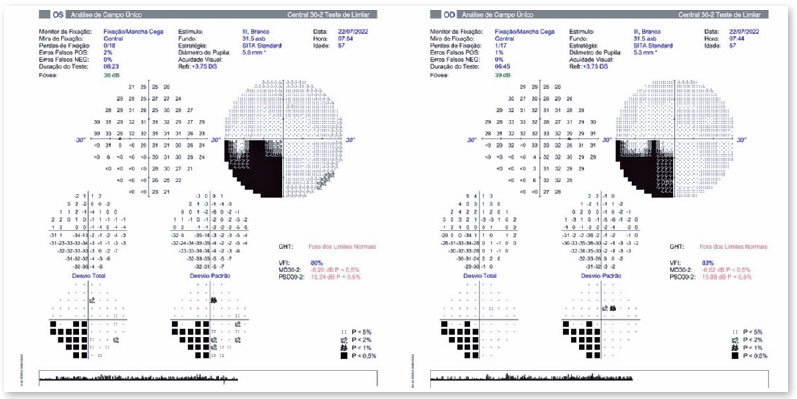
The visual field showed lower left quadrantanopia, sparing the macula (Figure 1). Optical coherence tomography of the nerve-fiber and ganglion-cell layers was within normal parameters. Magnetic resonance imaging showed an area of encephalomalacia superior to the right calcarine sulcus (Figure 2).
DISCUSSION
The presence of a left-homonymous defect in the visual field locates the defect as postchiasmatic to the right. The absence of pupillary defect and the absence of loss of nerve-fiber layer localizes the defect as postgeniculate. Inferior quadrantanopias are commonly found in parietal optic radiation lesions. However, the fact that this lesion spares the macula leads one to think of an occipital cortical lesion superior to the calcarine fissure, which was confirmed on imaging1.
REFERENCES
1. Levin LA chapter 12 - Topical Diagnosis of Chiasmal and Retrochiasmal Disorders. In Miller N, Subramanian P, Patel V, editores. Walsh and Hoyt clinical neurophthalmology - The essentials. Philadelphia: Wolters Kluwer; 2005. P 503-573
| AUTHOR INFORMATION |
|
 |
»Luciana da Cruz Noia https://orcid.org/0000-0003-2674-051X http://lattes.cnpq.br/7297139417211310 |
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
June 5, 2023.
Accepted on:
August 15, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket