

Carlos Augusto Moreira Neto; Gilberto Antonio Tesser Augusto
DOI: 10.17545/eOftalmo/2021.0014
ABSTRACT
Central retinal vein occlusion is the blockage of retinal blood circulation owing to obstruction of the central retinal vein. Depending to the degree of occlusion and retinal ischemia, it is classified into ischemic and non-ischemic forms. Central retinal vein occlusion leads to the development of important vascular alterations, increased inflammatory factors, and retinal edema. Diagnosis is made by ophthalmoscopy findings and complementary examinations. The clinical presentation varies from insidious painless unilateral vision loss to abrupt and profound vision loss. Neovascular glaucoma is the most severe complication, and macular edema is the most common complication. Treatment includes the identification and correction of systemic vascular risk factors. Intravitreal injections of antiangiogenics and corticosteroids can help improve final visual acuity. In this review article, we describe the main clinical and therapeutic aspects of central retinal vein occlusion.
Keywords: Central retinal vein; Retinal vein occlusion; VEGF; Intravitreal injections; Macular edema.
RESUMO
A Oclusão da Veia Central da Retina é o bloqueio da circulação sanguínea retiniana por obstrução da veia central da retina. Subdivide-se em isquêmica e não isquêmica de acordo com o grau de oclusão e de isquemia retiniana. O evento obstrutivo proporciona o desenvolvimento de alterações vasculares importantes, aumento de fatores inflamatórios e edema retiniano. O diagnóstico é feito pelos achados oftalmoscópicos e exames complementares. A apresentação clínica é variável, desde perda visual unilateral indolor insidiosa até perda abrupta e profunda da visão. Glaucoma neovascular é a complicação mais severa. A complicação mais comum é o edema macular. O tratamento inclui identificação e correção dos fatores de risco vasculares sistêmicos. O uso de injeções intravítreas de antiangiogênicos e corticoides pode auxiliar na melhora da acuidade visual final. Neste artigo de revisão descreveremos os principais aspectos clínicos e terapêuticos da oclusão venosa central retiniana.
Palavras-chave: Veia central da retina; Oclusão da veia retiniana; VEGF; Injeções intravítreas; Edema macular.
INTRODUCTION
Central retinal vein occlusion (CRVO) occurs due to blockage of retinal blood circulation resulting from obstruction of the central retinal vein, and consequently of its branches, in the region of the cribriform plate or in a location immediately posterior to it1.
Retinal vein occlusion (RVO) is the second leading cause of vascular blindness, surpassed only by diabetic retinopathy. In 2008, it was estimated that approximately 16.4 million adults had some type of RVO, and 2.5 million were affected by CRVO2.
The worldwide prevalence of CRVO is approximately 0.08%, with a similar distribution among different ethnicities and sexes. Its risk increases with increasing age2. However, one study reported that Black people were 58% more likely to develop CRVO than White people3.
The best predictor of RVO development is prior episodes in the contralateral eye. The risk of contralateral involvement in individuals with CRVO is approximately 1% per year4.
Cardiovascular risk factors such as atherosclerosis, hypertension, and diabetes are commonly associated with all types of RVOs. However, vein occlusions can also be secondary to other processes, such as inflammation, vasospasm, or compression5.
CRVO is correlated with glaucoma, sleep apnea, thrombophilia, and homocystinuria6. A study demonstrated that smoking, alcoholism, hyperopia, and pseudophakia increased the risk of RVO7.
Blood hyperviscosity, which is observed in myeloproliferative disorders, may also be associated with CRVO. Inflammatory conditions that cause systemic vasculitis (Behçet’s disease, lupus, polyarteritis nodosa) and hypercoagulation states (hyperhomocysteinemia, antiphospholipid syndrome, deficiency of proteins C or S or antithrombin III) have also been described as risk factors for RVO, particularly in young patients, although this is rare8,9.
The incidence of CRVO increases with age, and most affected individuals are aged ≥50 years10. CRVO in young adults is uncommon and only 10%-15% of patients are aged <40 years11.
METHODS
This is a narrative literature review of studies retrieved from electronic databases (PubMed/MEDLINE, Google Scholar, and SCIELO) using the descriptors “central retinal vein,” “retinal vein occlusion,” “VEGF,” and “macular edema.” These terms were used in Portuguese and English, individually and in combination. The authors selected the articles considered most important, and their information was extracted to compose the textual base and describe the most relevant aspects of CRVO.
Pathophysiology
The pathogenesis of CRVO is multifactorial and involves alterations in hematological factors, compression, and abnormalities in the vessel wall. The existence of an intimate anatomical relationship between the intima layers of the central artery and the central vein of the retina in the posterior region of the cribriform plate can lead to venous compression and formation of fibrin and platelet thrombi, consequently resulting in vessel obstruction12.
RVO can cause acute endothelial cell apoptosis, pericyte damage, and increased vascular permeability. Chronic ischemia and edema appear as the final outcomes of abnormal endothelial cell turnover and retinal hypersensitivity to hypoxia13.
The increase in intraluminal pressure, as a consequence of the obstruction, triggers the production of inflammatory mediators, including vascular endothelial growth factor (VEGF), and compromises the internal blood–retinal barrier. This, in turn, promotes transudation of vessels, leading to optic nerve edema, intraretinal hemorrhages in the four retinal quadrants, and macular edema. When neovascularization occurs, it can result in neovascular glaucoma and vitreous hemorrhage14,15.
Classification
CRVO can be classified into two forms: the ischemic and non-ischemic forms. Approximately 80% of patients with CRVO suffer from the non-ischemic form, which is characterized by venous stasis retinopathy and an obstruction posterior to the cribriform plate. This location could justify a milder retinopathy owing to the presence of more collateral venous channels. In ischemic CRVO, with characteristics of hemorrhagic retinopathy, venous obstruction occurs at the level of the cribriform plate or immediately posterior to it. Few collateral venous channels are present to aid in drainage, and the retina suffers from extensive ischemia due to reduced perfusion pressure. Further, in some cases the non-ischemic form can progress to the ischemic form, likely due to either reduced retinal perfusion during sleep or thrombus migration to a region closer to the cribriform plate16.
The classification of CRVO subtypes is based on fluorescein angiography (FA) findings. Non-ischemic CRVO is characterized by an ischemic area of <10 disc areas and the absence of retinal neovascularization on examination. Ischemic CRVO is characterized by retinal or iris neovascularization with a large ischemic area (>10 disc areas) and a larger number of hemorrhages4.
This classification has been useful for use in studies. However, with the advent of widefield angiography, it is possible to better assess the large peripheral nonperfusion areas present in cases of CRVO17. It is suggested that peripheral ischemia rates of >35% are an angiographic criterion for classifying CRVO cases as ischemic CRVO18.
Signs and symptoms
Patients with CRVO should undergo a complete eye examination. Ocular symptoms at the onset of CRVO are variable, ranging from no symptoms to severe reduction in visual acuity (VA). Vision loss is usually sudden and unilateral, but it may be gradual, progressing to definitive over a period of days to weeks19.
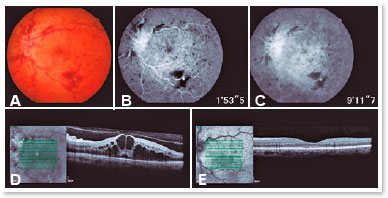
The examiner must determine which presentation subtype of CRVO is developing. The non-ischemic form is the most common clinical presentation. In this form, unilateral and sudden vision blurring are observed, with moderate impairment of the VA (20/200 or better). On fundoscopy, the branches of the central retinal vein appear tortuous and dilated and are accompanied by “candle-flame” hemorrhages in all quadrants, but more markedly in the periphery20 (Figure 1A).
Almost all patients with ischemic CRVO have an initial VA of 20/200 or worse, and approximately half have significant peripheral visual field involvement. Most also exhibit a relative afferent pupillary defect (RAPD), which can be a sensitive and specific indicator of ischemic CRVO6.
In the ischemic form, fundoscopy features are more prominent, marked by significant engorgement and tortuosity of the branches of the central retinal vein, in addition to “cotton-wool” exudates associated with extensive hemorrhages. The presence of “cotton-wool” exudates reflects infarction foci in the nerve fiber layer and neovascularization of the anterior or posterior segment in more advanced stages21.
Capillary congestion can result in macular and optic nerve edema. Hence, complaints may include metamorphopsia associated with reduced VA6.
Complementary examinations
The evaluation of patients with RVO should include a comprehensive investigation of medical history and laboratory findings to identify cardiovascular risk factors. Suggested tests include electrocardiography, protein electrophoresis, and determination of complete blood count, erythrocyte sedimentation rate, urea, electrolytes, creatinine, blood glucose, lipid profile, thyroid function, and blood pressure22.
In recent years, the hypothesis that coagulation disorders could be related to RVO has been discussed23. Tests for coagulation disorders can be performed in selected cases, such as those involving young patients (<50 years old), bilateral venous occlusion, and history of coagulation disorders or thrombophilia22. In the case of thrombophilia, a study suggested that the investigation should focus on factor XII, factor V Leiden deficiency, homocysteinemia, antiphospholipid antibody, and deficiency of anticoagulant proteins C and S24.
Ophthalmological imaging tests
Ocular investigations for CRVO usually include FA, optical coherence tomography (OCT), and, more recently, optical coherence tomography angiography (OCTA).
Fluorescein angiography (FA)
FA is a useful and objective tool for evaluating retinal circulation through the use of intravenous fluorescein contrast. Fluorescein leaks only from physiologically abnormal vessels and capillaries, and the amount of leakage depends on the severity of the occlusion25.
In cases of CRVO, FA enables the analysis of poor peripheral capillary perfusion and macular ischemia and the detection of neovascularization, even distinguishing the latter from the formation of collateral circulation6.
In CRVO, FA demonstrates normal filling of the choroid, but there may be a variable delay in retinal vascular filling caused by venous flow congestion. In late phases, FA presents a variable pattern of uptake in the optic nerve head and retinal veins, which is associated with variable degrees of poor capillary perfusion and extravasation in the macular region1 (Figures 1B and 1C).
FA is useful for providing information about the capillary bed of the retina (permeability or nonperfusion) and in differentiating between the ischemic and non-ischemic forms of RVO. Other findings include late extravasation in the macular area and in the filling of veins. Macular edema usually appears as hyperfluorescence in radial cystic cavities, forming a “petaloid” pattern. The presence of peripheral nonperfusion is a characteristic of ischemic RVO and is an important risk factor for neovascularization. Macular nonperfusion is correlated with a poor visual prognosis, and improving VA can be difficult, even with treatment for macular edema26.
Optical coherence tomography (OCT)
OCT is a noninvasive retinal examination method that, through sectional images, enables the identification of retinal layers in near-histological detail27. It is an important test to confirm and monitor the presence of macular edema6.
In cases of CRVO, OCT typically reveals intraretinal cysts (Figure 1D), retinal thickening, and occasionally submacular fluid. As for structural alterations, there may be a loss of the relationship between the internal and external segments of the photoreceptors and a distortion of the architecture of the nuclear and internal plexiform layers1,27.
Optical coherence tomography angiography (OCTA)
OCTA is a recent, noninvasive imaging technique that was developed to enable the study of retinal microvessels without contrast injection. The movement of red blood cells within retinal capillaries is used as an intrinsic contrast medium to generate flow images. OCTA provides images of the capillary network of both the superficial and deep retina, with detailed visualization of the avascular zone of the fovea and the possibility of constructing a three-dimensional vascular map of retinal circulation28.
OCTA demonstrates the characteristic findings of venous occlusions seen in FA, such as decreased capillary perfusion, macular edema, vascular dilation, enlarged avascular zone of the fovea, and collateral venous circulation29.
Monitoring and prognosis
Ophthalmological follow-up should prevent and identify complications caused by retinal ischemia, such as neovascular glaucoma, vitreous hemorrhage, and macular edema.
In ischemic cases, follow-up should be monthly in the first semester, to monitor macular edema and identify signs of neovascularization of the anterior segment. Follow-up of the eyes with significant ischemia after the first semester should be done every 3 months for 1 year. In non-ischemic cases, a quarterly follow-up is suggested for the first 6 months. For all patients, subsequent follow-up depends on the treatment performed and the complications present, but in cases with no complications, it is usually not necessary after 2 years. Macular edema may recur for several years; hence, follow-up beyond recommendations may be necessary for long-term VA maintenance30.
Initial VA is usually the most reliable factor to predict the severity and visual prognosis in eyes with CRVO27.
In cases of patients with VA 20/60 or better, VA tends to remain unaltered; VA between 20/80 and 20/200 has a variable clinical course; VA worse than 20/200 is likely to show no improvement4.
The prognosis of ischemic CRVO is poor owing to the presence of macular ischemia and an increased risk of neovascularization. In one study, the cumulative incidence of neovascularization was 52% and neovascular glaucoma development was 34% at 9 months after ischemic CRVO31.
Conversion from the non-ischemic to the ischemic form usually occurs in one third of patients within 3 years32.
The main factors related to the development of neovascular glaucoma are a history of arterial hypertension, low VA, or RAPD at the onset of the condition. If VA worsens or RAPD emerges, the possibility of conversion to the ischemic form must be considered and the patient must be monitored closely33.
TREATMENT
Interventions performed in cases of CRVO focus on occlusion sequelae, which include macular edema and retinal ischemia1.
Current treatment options include the use of laser, surgical interventions, and intravitreal injections of corticosteroids and VEGF inhibitors34.
To date, there is no consistent evidence that clinical treatments can favorably alter the natural course of CRVO. There is no evidence that the use of antiplatelet agents, anticoagulants, thrombolytic agents, or hemodilution are effective in improving VA35.
The use of antiplatelet agents or systemic anticoagulants for the treatment of CRVO does not show benefits and has been associated with worse outcomes in terms of final VA, greater loss of visual field, and worsening of retinal hemorrhage36.
Optimizing the control of arterial hypertension, diabetes, dyslipidemia, and intraocular pressure are important for controlling systemic risk factors for CRVO and other consequences causing damage to target organs37.
Most surgical procedures require further studies and should not be routinely indicated owing to possible complications. The use of thrombolytics by injection into the ophthalmic artery has not yet demonstrated obvious efficacy. Further, other surgical techniques such as peeling of the internal limiting membrane, radial neurotomy, and decompression of the optic nerve sheath are not completely effective35.
The formation of chorioretinal anastomoses using a laser has variable results (33%–88% success in VA improvement), but it remains an experimental therapy38.
The development of severe vitreous hemorrhage or tractional retinal detachment can be controlled using vitrectomy techniques39.
Macular edema and neovascularization
Macular edema caused by capillary fluid leakage in the central macular area is the most common cause of vision loss in patients with RVO40.
In non-ischemic CRVO, spontaneous resolution of the macular edema has been observed over time in approximately 30% of eyes41.
The isolated use of laser in a macular grid has not shown great benefit in improving VA, even though it significantly reduces extravasation on angiography42.
However, studies have reported beneficial effects from the combined use of laser and intravitreal injections in improving VA in cases of CRVO, in addition to better therapeutic responses and fewer interventions43.
The use of a macular grid can be considered in patients with persistent macular edema after 3-4 monthly FA-guided injections of anti-VEGF agents to determine the sites of ischemia and extravasation that could benefit from laser treatment44.
Prophylactic panretinal photocoagulation is no longer recommended for ischemic CRVO as it does not prevent iris neovascularization. However, laser photocoagulation should be performed when neovascularization occurs in the anterior segment, the optic disc, or the retina 8.
When regular follow-up is impractical, prophylactic panretinal photocoagulation may be advisable30.
The use of intravitreal or intracameral anti-VEGF agents can significantly aid in reducing retinal and anterior segment neovascularization45.
In cases of established neovascular glaucoma and blindness, the goal should be pain control with the use of topical steroids and atropine. However, if there is a prognosis of preserved vision, intraocular pressure control with hypotensive eye drops or surgery should be sought40.
Effective benefits in the management of macular edema have recently been demonstrated with the use of intravitreal injections of anti-VEGF agents (bevacizumab, ranibizumab, and aflibercept) and corticosteroids (triamcinolone and dexamethasone). Both classes of medication have important anti-inflammatory and antiproliferative mechanisms that help to reduce macular edema and neovascularization and improve VA46.
Anti-VEGF agents
There are three anti-VEGF agents available for use: bevacizumab (off-label), ranibizumab, and aflibercept. Currently, intravitreal therapy with anti-VEGF agents is considered the first-line therapy for the treatment of macular edema associated with RVO47.
In eyes with RVO, structural changes in the retinal venous system result in reduced blood flow, variable levels of hypoxia, and a subsequent sharp increase in intravitreal VEGF levels48,49.
Intravitreal VEGF levels have been shown to correlate with the severity of clinical findings50.
Ranibizumab
Ranibizumab is a recombinant humanized monoclonal antibody capable of inhibiting the biological activity of all VEGF-A isoforms. It was developed specifically for intravitreal use and is approved for the treatment of macular edema related to RVO51.
In the CRUISE and BRAVO studies, monthly 0.5 mg ranibizumab injections significantly improved visual function in patients with RVO after 6 months of follow-up (respectively, 18.3 and 14.9 ETDRS letters vs. 7.3 and 0.8 letters in the control group), in addition to improving the mean central foveal thickness (345 µm and 442 µm vs. 158 µm and 168 µm in the control group)47,51.
Although macular edema resolution occurs in approximately half of the patients with RVO with ranibizumab treatment, in cases of CRVO, a substantial number of individuals require frequent injections, even years after the initial treatment52.
Aflibercept
Aflibercept is a fusion protein composed of domains of human VEGF receptors 1 and 2 fused with a segment of human IgG. It is capable of inhibiting all VEGF-A isoforms. It has a long duration and high affinity for VEGF-B and placental growth factor53.
Two randomized clinical trials (GALILEO and COPERNICUS) assessed the use of intravitreal aflibercept versus sham injections for the treatment of macular edema secondary to CRVO and reported similar results. Both studies demonstrated the efficacy of aflibercept in improving the anatomical and visual outcomes of patients with macular edema associated with CRVO in the first 6 months under fixed monthly administration of aflibercept54,55. In the GALILEO study, 60.2% and 22.1% of patients in the treatment and placebo groups, respectively, demonstrated a gain of at least 15 letters after 6 months of treatment54.
In the COPERNICUS study, there was a gain of 15 letters in 56% of the treated eyes compared with 12% of the sham treatment eyes after 6 months of treatment. Further, there were no cases of neovascularization or photocoagulation in those treated with aflibercept. Hence, these studies not only demonstrated the benefits of treatment over natural progression but also depicted superior results with the early treatment of CRVO-related macular edema with aflibercept55.
Bevacizumab
Bevacizumab is a humanized antibody that blocks all VEGF-A isoforms. Several studies have shown that the intravitreal injection of bevacizumab increased VA and concomitantly reduced central macular thickness56–58.
A large multicenter retrospective study involved the treatment of 44 eyes with 1.25 mg bevacizumab every 4–8 weeks during two years of follow-up while observing for any signs of macular edema. A mean gain of 3.5 ETDRS lines in 24 months was demonstrated, and the central macular thickness was reduced from 635 µm at baseline to 364 µm at the end of the study 59.
To date, bevacizumab has not been approved by the FDA for intraocular use owing to the lack of large randomized clinical trials and its use remains off-label60.
Corticosteroids
Corticosteroids are able to reduce edema by stabilizing vascular permeability, reducing inflammatory mediators, and indirectly blocking VEGF actions46.
Currently, two medications in this group are used for the treatment of macular edema associated with CRVO: intravitreal implants of dexamethasone (on-label use) and triamcinolone (off-label use)61,62.
Both these steroids are associated with clinically significant increases in intraocular pressure and cataract progression. Triamcinolone is a cost-effective treatment for a select groups of patients, such as those with pseudophakia or preexisting cataracts who may soon require cataract surgery46.
The SCORE–CRVO study sought to assess the improvement in macular edema associated with CRVO after intraocular application of triamcinolone at doses of 1 mg and 4 mg in comparison to a control group. A gain of ≥15 ETDRS letters was observed in 26.5% of patients who underwent intraocular application of 4 mg of triamcinolone after 12 months of follow-up, and the decrease in central macular thickness compared to baseline was greater in this group. However, the proportion of patients with central macular thickness of ≤250 µm was similar in the three groups at the end of 12 months63.
The GENEVA study evaluated the use of a dexamethasone implant (Ozurdex®) for the treatment of macular edema secondary to branch retinal vein occlusion (BRVO) and CRVO. This study demonstrated long-term effectiveness and significant improvement in VA in the groups using the medication (0.35 mg and 0.70 mg) compared to the control group64.
REFERENCES
1. McAllister IL. Central retinal vein occlusion: a review. Clin Exp Ophthalmol. 2012;40(1):48-58.
2. Rogers S, McIntosh RL, Cheung N, Lim L, Wang JJ, Mitchell P, et al. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010;117(2):313-9.
3. Stem MS, Talwar N, Comer GM, Stein JD. A longitudinal analysis of risk factors associated with central retinal vein occlusion. Ophthalmology. 2013;120(2):362-70.
4. The Central Vein Occlusion Study Group. Natural history and clinical management of central retinal vein occlusion. Arch Ophthalmol. 1997;115(4):486-91.
5. O’Mahoney PRA, Wong DT, Ray JG. Retinal Vein Occlusion and Traditional Risk Factors for Atherosclerosis. JAMA Ophthalmol. 2008;126(5):692-9.
6. Ip M, Hendrick A. Retinal Vein Occlusion Review. Asia Pac J Ophthalmol. 2018;7(1):40-5.
7. Thapa R, Bajimaya S, Paudyal G, Khanal S, Tan S, Thapa SS, et al. Prevalence, pattern and risk factors of retinal vein occlusion in an elderly population in Nepal: the Bhaktapur retina study. BMC Ophthalmol. 2017;17(1):162.
8. Karia N. Retinal vein occlusion: pathophysiology and treatment options. Clin Ophthalmol. 2010;4:809-16.
9. Wittström E. Central Retinal Vein Occlusion in Younger Swedish Adults: Case Reports and Review of the Literature. Open Ophthalmol J. 2017;11:89-102.
10. Mitchell P, Smith W, Chang A. Prevalence and Associations of Retinal Vein Occlusion in Australia: The Blue Mountains Eye Study. JAMA Ophthalmol. 1996;114(10):1243-7.
11. Marcucci R, Sofi F, Grifoni E, Sodi A, Prisco D. Retinal vein occlusions: a review for the internist. Intern Emerg Med. 2011;6(4):307-14.
12. Green WR, Chan CC, Hutchins GM, Terry JM. Central retinal vein occlusion: a prospective histopathologic study of 29 eyes in 28 cases. Trans Am Ophthalmol Soc. 1981;79:371-422.
13. Li J, Paulus YM, Shuai Y, Fang W, Liu Q, Yuan S. New Developments in the Classification, Pathogenesis, Risk Factors, Natural History, and Treatment of Branch Retinal Vein Occlusion. J Ophthalmol. 2017;2017:4936924.
14. Sauder G, Jonas JB. Ophthalmodynamometric Assessment of the Central Retinal Vein Collapse Pressure in Eyes with Retinal Vein Stasis or Occlusion. Invest Ophthalmol Vis Sci. 2003;44(13):352.
15. Noma H, Mimura T, Eguchi S. Association of Inflammatory Factors with Macular Edema in Branch Retinal Vein Occlusion. JAMA Ophthalmol. 2013;131(2):160-5.
16. Hayreh S. Retinal vein occlusion. Indian J Ophthalmol. 1994;42(3): 109-32.
17. Spaide RF. Peripheral areas of nonperfusion in treated central retinal vein occlusion as imaged by wide-field fluorescein angiography. Retina. 2011;31(5):829-37.
18. Thomas AS, Thomas MK, Finn AP, Fekrat S. Use of the ischemic index on widefield fluorescein angiography to characterize a central retinal vein occlusion as ischemic or nonischemic. Retina. 2019;39(6):1033-8.
19. Kooragayala LM, Pakaini V, Fong D, Charles S, Brown L, Roy Sr H. Central retinal vein occlusion. Disponível em: http://emedicinemedscape com/article/1223746-overview. 2005.
20. Hayreh S. Classification of Central Retinal Vein Occlusion. Ophthalmology. 1983;90(5):458-74.
21. Ehlers JP, Fekrat S. Retinal Vein Occlusion: Beyond the Acute Event. Surv. Ophthalmol. 2011;56(4):281-99.
22. Wong TY, Scott IU. Retinal-Vein Occlusion. N Engl J Med 2010; 363(22):2135-44.
23. Rehak M, Rehak J, Müller M, Faude S, Faude F, Siegemund A, et al. The prevalence of activated protein C (APC) resistance and factor V Leiden is significantly higher in patients with retinal vein occlusion without general risk factors. Thromb Haemost. 2008;99(11):925-9.
24. Kuhli-Hattenbach C, Scharrer I, Lüchtenberg M, Hattenbach L-O. Coagulation disorders and the risk of retinal vein occlusion. Thromb Haemost. 2010;103(02):299-305.
25. Kolar P. Definition and classification of retinal vein occlusion. Int J Ophthalmol Res. 2016;2(2):124-9.
26. Ho M, Liu DTL, Lam DSC, Jonas JB. Retinal vein occlusions, from basics to the latest treatment. Retina. 2016;36(3):432-48.
27. Lima VC, Yeung L, Castro LC, Landa G, Rosen RB. Correlation between spectral domain optical coherence tomography findings and visual outcomes in central retinal vein occlusion. Clin Ophthalmol. 2011;5:299-305.
28. Cardoso JN, Keane PA, Sim DA, Bradley P, Agrawal R, Addison PK, et al. Systematic Evaluation of Optical Coherence Tomography Angiography in Retinal Vein Occlusion. Am J Ophthalmol. 2016;163:93-107.
29. Mastropasqua R, Toto L, Di Antonio L, Borrelli E, Senatore A, Di Nicola M, et al. Optical coherence tomography angiography microvascular findings in macular edema due to central and branch retinal vein occlusions. Sci. Rep. 2017;7:40763.
30. Sivaprasad S, Amoaku WM, Hykin P, Sivaprasad S, Amoaku W, Williamson T, et al. The Royal College of Ophthalmologists Guidelines on retinal vein occlusions: executive summary. Eye. 2015;29(12):1633-8.
31. Hayreh SS, Zimmerman MB. Ocular neovascularization associated with central and hemicentral retinal vein occlusion. Retina. 2012;32(8):1553-65.
32. The Central Vein Occlusion Study Group. Baseline and Early Natural History Report: The Central Vein Occlusion Study. JAMA Ophthalmol. 1993;111(8):1087-95.
33. Rong AJ, Swaminathan SS, Vanner EA, Parrish RK. Predictors of Neovascular Glaucoma in Central Retinal Vein Occlusion. Am J Ophthalmol. 2019;204:62-9.
34. Bradshaw SE, Gala S, Nanavaty M, Shah A, Mwamburi M, Kefalas P. Systematic literature review of treatments for management of complications of ischemic central retinal vein occlusion. BMC Ophthalmol. 2016;16(1):104.
35. Mohamed Q, McIntosh RL, Saw SM, Wong TY. Interventions for Central Retinal Vein Occlusion: An Evidence-Based Systematic Review. Ophthalmology. 2007;114(3):507-19.
36. Hayreh SS, Podhajsky PA, Zimmerman MB. Central and Hemicentral Retinal Vein Occlusion: Role of Anti–Platelet Aggregation Agents and Anticoagulants. Ophthalmology. 2011; 118(8):1603-11.
37. Pulido JS, Flaxel CJ, Adelman RA, Hyman L, Folk JC, Olsen TW. Retinal vein occlusions preferred practice pattern® guidelines. Ophthalmology. 2016;123(1):P182-P208.
38. McAllister IL, Smithies LA, Previn V. Technique of laser chorioretinal anastomosis creation in central retinal vein occlusion and success rate with a new photocoagulator system. Retina. 2016;36(10):1971-8.
39. Bhagat N, Goldberg MF, Gascon P, Bell W, Haberman J, Zarbin MA. Central Retinal Vein Occlusion: Review of Management. Eur J Ophthalmol. 1999;9(3):165-80.
40. Kiire CA, Chong NV. Managing retinal vein occlusion. BMJ. 2012;344:e499.
41. McIntosh RL, Rogers SL, Lim L, Cheung N, Wang JJ, Mitchell P, et al. Natural History of Central Retinal Vein Occlusion: An Evidence-Based Systematic Review. Ophthalmology. 2010;117(6):1113-23.
42. The Central Vein Occlusion Study Group. Evaluation of Grid Pattern Photocoagulation for Macular Edema in Central Vein Occlusion: The Central Vein Occlusion Study Group M Report. Ophthalmology. 1995;102(10):1425-33.
43. Shah NJ, Shah UN. Long-term effect of early intervention with single intravitreal injection of bevacizumab followed by panretinal and macular grid photocoagulation in central retinal vein occlusion (CRVO) with macular edema: A pilot study. Eye. 2011;25(2):239-44.
44. Berger AR, Cruess AF, Altomare F, Chaudhary V, Colleaux K, Greve M, et al. Optimal Treatment of Retinal Vein Occlusion: Canadian Expert Consensus. Ophthalmologica. 2015;234(1):6-25.
45. Chalam KV, Gupta SK, Grover S, Brar VS, Agarwal S. Intracameral Avastin Dramatically Resolves Iris Neovascularization and Reverses Neovascular Glaucoma. Eur J Ophthalmol. 2008;18(2):255-62.
46. Ford JA, Clar C, Lois N, Barton S, Thomas S, Court R, et al. Treatments for macular oedema following central retinal vein occlusion: systematic review. BMJ Open. 2014;4(2):e004120.
47. Brown DM, Campochiaro PA, Singh RP, Li Z, Gray S, Saroj N, et al. Ranibizumab for Macular Edema following Central Retinal Vein Occlusion: Six-Month Primary End Point Results of a Phase III Study. Ophthalmology. 2010;117(6):1124-33.
48. Funk M, Kriechbaum K, Prager F, Benesch T, Georgopoulos M, Zlabinger GJ, et al. Intraocular Concentrations of Growth Factors and Cytokines in Retinal Vein Occlusion and the Effect of Therapy with Bevacizumab. Invest Ophthalmol Vis Sci. 2009;50(3):1025-32.
49. Noma H, Funatsu H, Yamasaki M, Tsukamoto H, Mimura T, Sone T, et al. Aqueous humour levels of cytokines are correlated to vitreous levels and severity of macular oedema in branch retinal vein occlusion. Eye. 2008;22(1):42-8.
50. Boyd SR, Zachary I, Chakravarthy U, Allen GJ, Wisdom GB, Cree IA, et al. Correlation of Increased Vascular Endothelial Growth Factor With Neovascularization and Permeability in Ischemic Central Vein Occlusion. JAMA Ophthalmol. 2002;120(12):1644-50.
51. Campochiaro PA, Heier JS, Feiner L, Gray S, Saroj N, Rundle AC, et al. Ranibizumab for Macular Edema following Branch Retinal Vein Occlusion: Six-Month Primary End Point Results of a Phase III Study. Ophthalmology. 2010;117(6):1102-12.
52. Campochiaro PA, Sophie R, Pearlman J, Brown DM, Boyer DS, Heier JS, et al. Long-term Outcomes in Patients with Retinal Vein Occlusion Treated with Ranibizumab: The RETAIN Study. Ophthalmology. 2014;121(1):209-19.
53. Holash J, Davis S, Papadopoulos N, Croll SD, Ho L, Russell M, et al. VEGF-Trap: A VEGF blocker with potent antitumor effects. Proc Natl Acad Sci U S A. 2002;99(17):11393.
54. Korobelnik J-F, Holz FG, Roider J, Ogura Y, Simader C, Schmidt-Erfurth U, et al. Intravitreal Aflibercept Injection for Macular Edema Resulting from Central Retinal Vein Occlusion: One-Year Results of the Phase 3 GALILEO Study. Ophthalmology. 2014;121(1):202-8.
55. Heier JS, Clark WL, Boyer DS, Brown DM, Vitti R, Berliner AJ, et al. Intravitreal Aflibercept Injection for Macular Edema Due to Central Retinal Vein Occlusion: Two-Year Results from the COPERNICUS Study. Ophthalmology. 2014;121(7):1414-20.
56. Epstein DL, Algvere PV, von Wendt G, Seregard S, Kvanta A. Bevacizumab for Macular Edema in Central Retinal Vein Occlusion: A Prospective, Randomized, Double-Masked Clinical Study. Ophthalmology. 2012;119(6):1184-9.
57. Epstein DL, Algvere PV, von Wendt G, Seregard S, Kvanta A. Benefit from Bevacizumab for Macular Edema in Central Retinal Vein Occlusion: Twelve-Month Results of a Prospective, Randomized Study. Ophthalmology. 2012;119(12):2587-91.
58. Zhang H, Liu Z-L, Sun P, Gu F. Intravitreal Bevacizumab for Treatment of Macular Edema Secondary to Central Retinal Vein Occlusion: Eighteen-Month Results of a Prospective Trial. J Ocul Pharmacol Ther. 2011;27(6):615-21.
59. Wu L, Arevalo JF, Berrocal MH, Maia M, Roca JA, Morales-Cantón V, et al. Comparison of two doses of intravitreal bevacizumab as primary treatment for macular edema secondary to central retinal vein occlusion: Results of the Pan American Collaborative Retina Study Group at 24 Months. Retina. 2010;30(7):1002-11.
60. Jiang Y, Mieler WF. Update on the Use of Anti-VEGF Intravitreal Therapies for Retinal Vein Occlusion. Asia Pac J Ophthalmol. 2017;6(6):546-53.
61. Park SP, Ahn JK. Changes of aqueous vascular endothelial growth factor and interleukin-6 after intravitreal triamcinolone for branch retinal vein occlusion.Clin Experiment Ophthalmol. 2008;36(9):831-5.
62. Ho M, Liu DTL, Lam DSC, Jonas JB. Retinal vein occlusions, from basics to the latest treatment. Retina. 2016;36(3):432-48.
63. Ip MS, Scott IU, VanVeldhuisen PC, Oden NL, Blodi BA, Fisher M, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 5. Arch Ophthalmol. 2009;127(9):1101-14.
64. Haller JA, Bandello F, Belfort R, Jr., Blumenkranz MS, Gillies M, Heier J, et al. Dexamethasone Intravitreal Implant in Patients with Macular Edema Related to Branch or Central Retinal Vein Occlusion: Twelve-Month Study Results. Ophthalmology. 2011;118(12):2453-60.
AUTHOR’S INFORMATION


Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose
Funding: No specific financial support was available for this study
Conflitos de Interesse: Declaram não haver
Received on:
June 16, 2020.
Accepted on:
November 2, 2020.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket