

Reinaldo Ramalho1; Antonio Marcelo Barbante Casella2; Lorena Aparecida Galhardo Ribeiro3; Claudio Dalloul4; Milton Ruiz Alves5
DOI: 10.17545/eoftalmo/2018.0019
ABSTRACT
OBJECTIVE: To describe the impact of choroidal neovascular age-related macular degeneration (nAMD) on vision-related quality of life (VRQoL) in a sample of Brazilian patients, demonstrate the ability of the NEI-VFQ 25 to evaluate the impact of treatment for nAMD on VRQoL, and make recommendations for incorporating the NEI-VFQ 25 into routine clinical practice.
METHODS: This observational clinical study included 87 patients clinically diagnosed with nAMD between September 2013 and November 2016 at three ophthalmology referral centers in São Paulo and Paraná (Brazil). At the end of the treatment, a validated Portuguese-language version of the NEI-VFQ 25 was self-administered, covering 12 domains. The findings were correlated with age, gender, disease laterality, and best-corrected visual acuity (VA) of the best eye and the worst eye.
RESULTS: All the measured variables affected VRQoL, especially laterality, followed by age and gender. VA of the best eye significantly affected the greatest number of domains. In contrast, VA of the worst eye was nonsignificant in all domains.
CONCLUSIONS: In nAMD patients, maintaining VA (Snellen) ≥0.5 in the best eye is essential for sustained VRQoL, regardless of VA in the worst eye. The incorporation of the NEI-VFQ 25 into routine clinical practice is strongly recommended.
Keywords: Macular degeneration; Quality of life; Assessment; Chronic disease.
RESUMO
OBJETIVO: Descrever o impacto de degeneração macular choroidal neovascular relacionada à idade (nAMD) sobre a qualidade de vida visual (QVV) em uma amostra de pacientes brasileiros, demonstrar a relevência do questionário NEI-VFQ 25 à avaliação do impacto do tratamento para nAMD sobre a QVV, e fazer recomendações para a incorporação do NEI-VFQ 25 à rotina clínica.
MÉTODOS: O presente estudo observacional incluiu 87 pacientes diagnosticados clinicamente com nAMD entre setembro de 2013 e novembro de 2016 em três centros de oftalmologia em São Paulo e Paraná. Ao fim do tratamento, o NEI-VFQ 25 (validado para a língua portuguesa) foi auto-aplicado, cobrindo 12 domínios. Os achados foram correlacionados com idade, gênero, lateralidade e acuidade visual (AV) no melhor e no pior olho.
RESULTADOS: Todas as variáveis mensuradas influenciaram a QVV, especialmente a lateralidade, seguida por idade e gênero. A AV do melhor olho foi a variável que influenciou significativamente o maior número de domínios relacionados à QVV; já a AV do pior olho não foi significante para nenhum domínio.
CONCLUSÕES: Em pacientes com nAMD, a manutenção de uma AV (Snellen) de ≥0.5 no melhor olho é fundamental para uma QVV sustentada, independentemente da AV no pior olho. A incorporação do NEI-VFQ 25 à rotina clínica é fortemente recomendada.
Palavras-chave: Degeneração Macular; Qualidade de vida; Doença crônica.
RESUMEN
OBJETIVO: Describir el influjo de la degeneración macular coroidal neovascular asociada a la edad (nAMD) sobre la cualidad de vida visual (QVV) en una amuestra de pacientes brasileños, demonstrar la relevancia de la encuesta NEI-VFQ 25 para la evaluación del impacto de la terapia para la nAMD sobre la QVV, además de hacerse recomendaciones a la incorporación de la encuesta NEI-VFQ 25 a la rutina clínica.
MÉTODOS: el presente estudio de observación incluye 87 pacientes diagnosticados clínicamente con nAMD entre los meses de septiembre de 2013 y noviembre de 2016 en tres centros de oftalmología en São Paulo y en Paraná. Al fin del tratamiento, la NEI-VFQ 25 (validada para la lengua portuguesa) fue aplicada de manera personal, alcanzando 12 dominios. Las respuestas encontradas se han correlacionado con edad, género, lateralidad y acuidad visual (AV) en el mejor y en el peor ojo.
RESULTADOS: Todas las variables medidas influenciaron la QVV, sobretodo la lateralidad, seguida por edad y género. La AV del mejor ojo fue la variable que influyó significativamente un número más grande de dominios relacionados a la QVV; ya la AV del peor ojo no mostró resultado significante para ningún de los dominios.
CONCLUSIONES: En pacientes con nAMD, la manutención de una AV (Snellen) de ≥0.5 en el mejor ojo es fundamental para una QVV que se sostenga, independientemente de la AV en el peor ojo. La incorporación de la NEIVFQ 25 a la rutina clínica se recomienda fuertemente.
Palabras-clave: Degeneración Macular; Calidad de Vida; Enfermedad Crónica.
INTRODUCTION
The Brazilian population is aging rapidly. In fact, Brazil now boasts having the world’s sixth-largest absolute number of citizens over 60 years of age1,2. This age range is associated with a significant increase in chronic degenerative diseases, including age-related macular degeneration (AMD)―the primary factor responsible for the severe and irreversible loss of visual acuity (VA)3. In its early stage, AMD is characterized by drusen and pigmentary changes, while late-stage AMD is classified into two subtypes: geographic atrophy and choroidal neovascularization (nAMD)4. Although only 10%–20% of AMD cases are classified as nAMD, this subtype accounts for 80%–90% of AMD-related blindness5.
Visual loss is correlated with morbidity and mortality in the elderly due to both the increased risk of falls, disability, and depression, and greater difficulty with daily activities6-9. In this scenario, VA is not as reliable a parameter of visual impairment8,9 as is vision-related quality of life (VRQoL). The latter may be quantified with the National Eye Institute Visual Functioning Questionnaire 25 (NEI-VFQ 25), with emphasis on daily activities6-11.
Antiangiogenic therapy [intravitreal administration of vascular endothelial growth factor (VEGF) inhibitors] is currently the treatment of choice for nAMD12-17. However, due to its prohibitive cost, access to treatment is limited in public healthcare. Improving the access of nAMD patients to antiangiogenic therapy in the Brazilian public health setting requires addressing a range of ethical and bioethical resource allocation issues. This strategy would make little sense unless it could be shown that the rehabilitation of nAMD patients had a significant influence on their VRQoL.
The primary objective of this study was to describe the impact of treatment for nAMD on VRQoL in a sample of Brazilian patients, explore the association between VRQoL and the parameters age, sex, and laterality, and determine the importance of VA of both the best eye (VA-BE) and the worst eye (VA-WE). The secondary objective was to assess the ability of the NEI-VFQ 25 to evaluate the impact of antiangiogenic therapy on VRQoL and make recommendations for incorporating the NEI-VFQ 25 into routine clinical practice.
METHODS
The sample of this observational clinical study consisted of 87 nAMD patients of both genders who submitted to retinal evaluation at three Brazilian ophthalmology referral centers―two in São Paulo (Araras; São José do Rio Preto), and one in Paraná (Londrina)―between September 2013, and November 2016.
Patient eligibility requirements for the study included that they give their informed written consent, be at least 50 years old, and have a clinical diagnosis of nAMD confirmed by optical coherence tomography and retinography. Also, they must follow the treat-and-extend protocol outlined in the LUCAS trial14 or the PrONTO protocol16, using aflibercept (Eylea®, Regeneron Pharmaceuticals Inc., Rensselaer, USA) or ranibizumab (Lucentis®, Novartis Pharma Stein AG, Stein, Switzerland).
Patients were excluded who had less than one year of follow-up or a history of non-AMD-related ocular disease potentially compromising VA (i.e., uncontrolled glaucoma, ischemic optic neuropathy, clinically significant diabetic macular edema, proliferative diabetic retinopathy, active uveitis, angioid streaks, signs of myopic choroiditis, and refraction greater than -8 D on the most recent prescription).
Study parameters included age, gender, number of anti-VEGF injections received, disease laterality, and best-corrected VA (Snellen) at the last follow-up visit.
The protocol was approved by the Research Ethics Committee of the University of São Paulo Medical School and filed under entry #253/2015.
NEI-VFQ 25
At the end of treatment, a validated, Portuguese-language version of the NEI-VFQ 2518 was self-administered that covered 12 domains: general health, general vision, ocular pain, near activities, distance activities, vision related social function, vision-related mental health, vision-related role difficulties, vision-related dependency, driving, color vision, and peripheral vision. The total score was calculated by averaging the 12 domains and ranged from 0 (worst possible function) to 100 (best possible function)18.
Cronbach’s alpha coefficients were calculated to evaluate the consistency and reliability of answers. A coefficient of ≥0.70 is recommended, although values above 0.60 are widely accepted in the literature19.
Associations between scores and dichotomous variables, such as gender (male/female) and laterality (unilateral/bilateral), were analyzed with the Mann-Whitney test. Associations with stratified age (<75 years; 75–84 years; >84 years) were evaluated with the Kruskal–Wallis test. Following confirmation of the assumption of homogeneity of variance and normality using scatter charts and normal curves, respectively, the impact of VA-BE (≥0.3 and <0.3) and VA-WE (≥1.0 and <1.0) on VRQoL was determined for each domain with a two-way fixed-effects ANOVA. We evaluated the effect of each eye, both independently and dependently (BE vs. WE). All statistical analyses were performed with the software SYSTAT v.12 (Systat Software Inc., Chicago, Illinois, USA). The level of statistical significance was set at 5% (α = 0.05).
RESULTS
Female gender was predominant in our sample of 87 Caucasian nAMD patients (n = 57; 65.5% vs. n = 30; 34.5%). The mean age and standard deviation was 78.4 ± 7.9 years. Age was distributed as follows: <75 years (n = 27; 31%), 75–84 years (n = 34; 39%), and >84 years (n = 26; 30%). Disease was more often unilateral than bilateral (n = 62; 72.9% vs. n = 25; 26.1%). The mean follow-up time was 76 ± 6.63 weeks. On average, patients with monocular and binocular disease received 9.2 ± 5.9 and 12.3 ± 7.9 anti-VEGF injections, respectively (overall mean: 9.84 ± 5.33). VA was 0.38 ± 0.19 (BE) and 0.13 ± 0.11 (WE).
Answers to the questionnaire met the basic criteria for internal consistency (Cronbach’s alpha coefficient >0.70), except for the domains ‘ocular pain’ and ‘driving’ (0.65). No coefficients could be calculated for the domains ‘general health,’ ‘general vision,’ ‘color vision,’ and ‘peripheral vision’ since they were represented by only one question on the NEI-VFQ 25.
All scores were above 60%, except for the domain ‘general health’ (49.43%). Mean scores above 90% were observed for ‘ocular pain’ (92.96%), ‘social function’ (90.23%), ‘color vision’ (93.60%), and ‘peripheral vision’ (90.52%). Mean scores in the range of 70%–80% were observed for ‘driving’ (77.96%), ‘dependency’ (74.71%), and ‘total score’ (72.26%). Mean scores in the range of 60%–70% were observed for ‘general vision’ (61.84%), ‘near activities’ (62.06%), ‘distance activities’ (65.85%), ‘mental health’ (63.5%), and ‘role difficulties’ (68.82%).
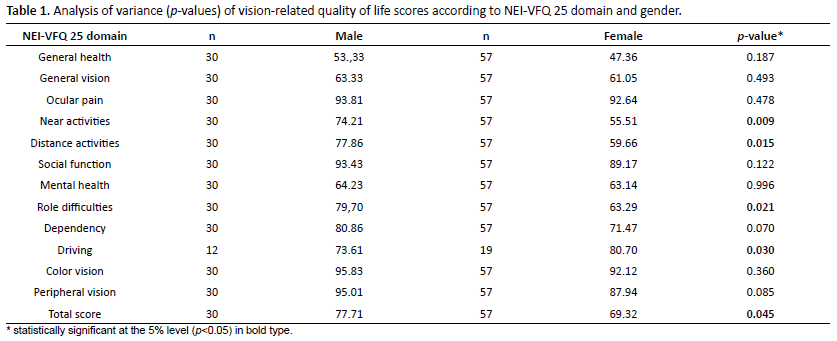
Males scored better than females on all domains, except for ‘driving,’ but the difference was only significant for ‘near activities,’ ‘distance activities,’ ‘role difficulties,’ ‘driving,’ and ‘total score’ (p < .05) (Table 1).
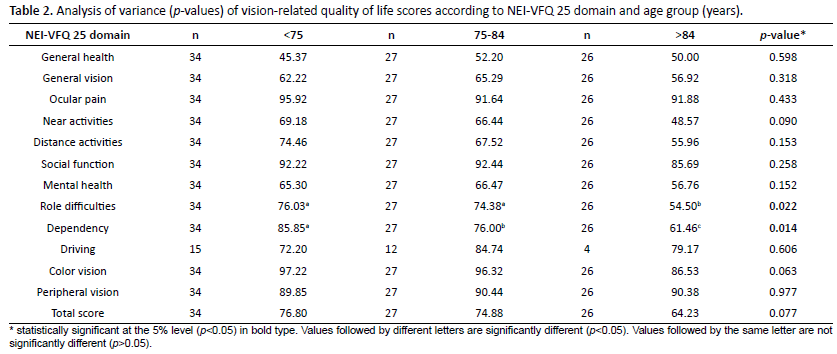
Mean scores for ‘role difficulties’ and ‘dependency’ were significantly associated with age (p < .01) (Table 2). Thus, ‘role difficulties’ scores were significantly higher for younger patients (≤84 years) than for patients >84 years (Table 2). Likewise, dependency scores varied significantly between the three age groups, with patients aged <75 years scoring the highest, followed by patients aged 75–84 years, and then by patients >84 years (Table 2).
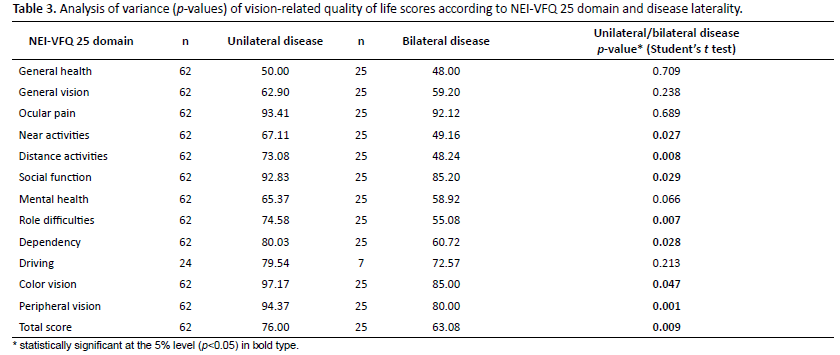
Mean scores for ‘near activities,’ ‘distance activities,’ ‘social function,’ ‘role difficulties,’ ‘color vision,’ ‘dependency,’ ‘peripheral vision,’ and ‘total score’ were significantly associated with disease laterality (p < .01). Thus, patients with bilateral disease had lower scores on all domains for which the association was statistically significant (Table 3).
The results of ANOVA revealed no significant interactions between BE and WE for any domain (Table 4). The impact of AV-BE was statistically significant for the dimensions ‘general vision,’ ‘near activities,’ ‘distance activities,’ ‘social function,’ ‘role difficulties,’ ‘dependency,’ ‘color vision,’ ‘peripheral vision,’ and ‘total score’ (p < .05) (Table 4).

Table 5 shows the individual effect of BE and WE for each domain since no significant interaction between the eyes was observed. The dimensions ‘general health,’ ‘mental health,’ ‘driving,’ and ‘ocular pain’ were not significantly associated with BE and WE. The independent influence of BE (between 0.43 and -23.64) was greater in all domains, except for ‘driving’ (Table 5). Scores were higher for VA-BE ≥0.3 than for VA-BE <0.3. The impact of WE on VRQoL was not significant. Mean scores were more than 20% lower for WE than for BE concerning ‘near activities’ (-23.64%), ‘distance activities’ (-22.34%), and ‘role difficulties’ (-20.91%) (Table 5).

DISCUSSION
The demographic profile of our sample (69% >75 years; 65.5% female) matched the normal distribution of a population of patients with AMD5. This fact is relevant since age can introduce bias into the interpretation of answers to questionnaires. The purpose of anti-VEGF therapy for nAMD is to inhibit choroidal neovascularization and maintain good vision for as long as possible. However, the situation requires a series of visits and injections5.
The NEI-VFQ 25 was used to identify associations between low vision and poor VRQoL in nAMD patients. In our opinion, the NEI-VFQ 25 is the best assessment tool available for this task. In the present study, VRQoL was affected by all variables tested, although some domains were more affected by VA than others.
The domains ‘distance activities,’ ‘near activities,’ ‘role difficulties,’ ‘driving,’ and ‘total score’ were significantly associated with gender (Table 1), while only two domains (‘role difficulties’ and ‘dependency’) were associated with age (Table 2). In comparison, AMD patients assessed by Szlyk et al.20 displayed poorer performance on the driving simulator, including delayed braking response times to stop signs, slower speeds, and both more lane boundary crossings and simulator accidents. AMD patients also displayed poorer overall on-road test performance, including having significantly more points deducted for driving too slowly and for not maintaining proper lane position.
Laterality was significantly associated with eight of the 12 domains on the NEI-VFQ 25 (Table 3). In these eight domains, scores were lower for patients with binocular disease. VA was the variable, which affected the greatest number of domains at statistically significant levels, i.e., the variable most strongly correlated with VRQoL. In two other studies, NEI-VFQ 25 scores were lower for binocular than for monocular AMD-related visual (vision) loss21,22. However, a study comparing 54 patients who had monocular blindness with 54 patients who had binocular blindness found higher levels of emotional distress in the former group, perhaps because of uncertainty regarding future disease progression23.
Lower scores in all domains of patients with bilateral nAMD are in agreement with the literature11,22. The most considerable difference between bilateral and monocular disease was observed for ‘role difficulties’ and ‘distance activities’ (>20%). As in other vision-threatening conditions, loss of near and far vision is a major cause of the loss of VRQoL among bilateral nAMD patients. In one study, AMD patients who reported poor adaptation to vision loss, especially concerning acceptance of and compensation for vision loss, had more depressive symptoms than better-adapted patients25. Role difficulties also severely compromise VRQoL and can aggravate depression in nAMD patients due to inability to work6-8. Activities commonly affected include meal preparation, traveling, cleaning, grooming, shopping, going out, navigating both steps and pavement curbs, noticing objects, hobbies, watching TV, reading, driving (especially night driving), and using low-vision devices26,27.
VA-BE influenced the highest number of VRQoL domains significantly, whereas VA-WE was not significant for all domains (Table 4). No significant interactions were found between BE and WE for any domain, suggesting BE and WE have independent effects on VRQoL21,22,24.
Patients with VA-BE ≥0.3 obtained higher NEI VF-25 scores than patients with VA-BE <0.3 (Table 5). Since VA-WE had no measurable influence on VRQoL in any domain, the maintenance of VA-BE ≥0.3 appears to be essential for sustained VRQoL in this population. Likewise, Berdeaux et al.24 found a strong correlation between VRQoL and VA-BE, suggesting the best eye be given treatment priority. This strategy is effective when VA-BE is <0.3, but the treatment of bilateral nAMD patients targeting only the best eye may underestimate the impact of low VA-WE on VRQoL. According to Hirneiss et al.28, VRQoL can be sustained or improved independently of which eye is given treatment priority.
The healthcare cost of a newly diagnosed nAMD patient may cost approximately USD 250,00029, a prohibitive cost in the public healthcare setting. Moreover, although currently available treatments for nAMD may preserve vision, they do not provide a cure for the disease. Our study shows that the maintenance of VA-BE ≥0.3 is essential for VRQoL, raising the question of whether resources and treatment for nAMD should be made available for both eyes, or primarily for the BE. Based on our findings, in nAMD patients with VA-BE <0.3, the best eye should be given priority to ensure VRQoL for as long as possible. Moreover, our study confirmed the ability of the NEI-VFQ 25 to evaluate the impact of treatment for nAMD on VRQoL. Thus, we strongly recommend the incorporation of this questionnaire into routine clinical assessments.
REFERENCES
1. Chaimowicz F. A saúde dos idosos brasileiros às vésperas do século XXI: problemas, projeções e alternativas. Rev Saúde Pública. 1997;31(2):184- 200.
2. Macedo BG, Pereira LSM, Castro ANBV, Camelo J, Sales PCD. Correlação entre acuidade visual e desempenho funcional em idosos com catarata. Geriatr Gerontol Aging. 2009;3(4):158-63.
3. Colijn JM, Buitendijk GHS, Prokofyeva E, Alves D, Cachulo ML, Khawaja AP, et al.; EYE-RISK consortium; European Eye Epidemiology (E3) consortium. Prevalence of Age-Related Macular Degeneration in Europe: The Past and the Future. Ophthalmology. 2017;124(12):1753-63.
4. Klein R, Klein BE, Linton KL. Prevalence of age-related maculopathy: the Beaver Dam Eye Study. Ophthalmology. 1992;99(6):933-43.
5. Ávila M, Garcia JMBB, Isaac DLC. Degeneração macular relacionada à idade: presente e futuro. e-Oftalmo.CBO: Rev Dig Oftalmol. 2015;1(2):1-2. DOI: 10.17545/e-oftalmo.cbo/2015.18 106 eOftalmo. 2018; 4(3): 100-107. CreativeCommons Atribuição-NãoComercial 4.0 Internacional Ramalho R, Casella AMB, Ribeiro LAG, Dalloul C, Alves MR
6. Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, Dolnak D, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893-900.
7. Borger PH, van Leeuwen R, Hulsman CA, Wolfs RC, van der Kuip DA, Hofman A, et al. Is there a direct association between age-related eye diseases and mortality? The Rotterdam Study. Ophthalmology. 2003;110(7):1292-6.
8. Yuzawa M, Fujita K, Tanaka E, Wang EC. Assessing quality of life in the treatment of patients with age-related macular degeneration: clinical research findings and recommendations for clinical practice. Clin Ophthalmol. 2013;7:1325-32.
9. Wang J, Xue Y, Thapa S, Wang L, Tang J, Ji K. Relation between Age-Related Macular Degeneration and Cardiovascular Events and Mortality: A Systematic Review and Meta-Analysis. Biomed Res Int. 2016;2016:8212063. DOI: 10.1155/2016/8212063.8212063
10. Margolis MK, Coyne K, Kennedy-Martin T, Baker T, Schein O, Revicki DA. Vision-specific instruments for the assessment of health-related quality of life and visual functioning: a literature review. Pharmacoeconomics. 2002;20(12):791-812.
11. Picoto M, Galveia J, Patrício S, Rodrigues A, Vaz F. Qualidade de vida relacionada com a visão em pacientes com degeneração macular relacionada à idade neovascular. Rev Bras Oftalmol. 2015;74(4):216-21.
12. Boyer DS, Heier JS, Brown DM, Francom SF, Ianchulev T, Rubio RG. A Phase IIIb study to evaluate the safety of ranibizumab in subjects with neovascular age-related macular degeneration. Ophthalmology. 2009;116(9):1731-9.
13. CATT Research Group, Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897-908.
14. Rayess N, Houston SK 3rd, Gupta OP, Ho AC, Regillo CD. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and-extend regimen. Am J Ophthalmol. 2015;159(1):3-8.e1.
15. Wykoff CC, Ou WC, Brown DM, Croft DE, Wang R, Payne JF, et al. Randomized Trial of Treat-and-Extend versus Monthly Dosing for Neovascular Age-Related Macular Degeneration. Ophthalmol Retina. 2017;1(4):314-21.
16. Lalwani GA, Rosenfeld PJ, Fung AE, Dubovy SR, Michels S, Feuer W, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol. 2009;148(1):43-58.e1.
17. Villegas VM, Aranguren LA, Kovach JL, Schwartz SG, Flynn HW Jr. Current advances in the treatment of neovascular age-related macular degeneration. Expert Opin Drug Deliv. 2017;14(2):273-82.
18. Simão LM, Lana-Peixoto MA, Araújo CR, Moreira MA, Teixeira AL. The Brazilian version of the 25-Item National Eye Institute Visual Function Questionnaire: translation, reliability and validity. Arq Bras Oftalmol. 2008;71(4):540-6.
19. Streiner DL. Being inconsistent about consistency: when coefficient alpha does and doesn’t matter. J Pers Assess. 2003;80(3):217-22.
20. Szlyk JP, Pizzimenti CE, Fishman GA, Kelsch R, Wetzel LC, Kagan S, et al. A comparison of driving in older subjects with and without age-related macular degeneration. Arch Ophthalmol. 1995;113(8):1033-40.
21. Dong LM, Childs AL, Mangione CM, Bass EB, Bressler NM, Hawkins BS, et al.; Submacular Surgery Trials Research Group. Health- and vision-related quality of life among patients with choroidal neovascularization secondary to age-related macular degeneration at enrollment in randomized trials of submacular surgery: SST report no. 4. Am J Ophthalmol. 2004;138(1):91-108.
22. Marback RF, Maia OO Jr, Morais FB, Takahashi WY. Quality of life in patients with age-related macular degeneration with monocular and binocular legal blindness. Clinics (Sao Paulo). 2007;62(5):573-8.
23. Williams RA, Brody BL, Thomas RG, Kaplan RM, Brown SI. The psychosocial impact of macular degeneration. Arch Ophthalmol. 1998;116(4):514-20.
24. Tolman J, Hill RD, Kleinschmidt JJ, Gregg CH. Psychosocial adaptation to visual impairment and its relationship to depressive affect in older adults with age-related macular degeneration. Gerontologist. 2005;45(6):747-53.
25. Vanoff SD, Sonn U, Lundgren-Lindqvist B, Steen SB. Disability in daily life activities and visual impairment: a population study of 85-year-old people living at home. Scand J Occup Ther. 2000;7(4):148-55.
26. Backman H, Williams R. Living with age-related macular degeneration. J Vis Impair Blind. 2002;96(5):345-8.
27. Berdeaux GH, Nordmann JP, Colin E, Arnould B. Vision-related quality of life in patients suffering from age-related macular degeneration. Am J Ophthalmol. 2005;139(2):271-9.
28. Hirneiss C, Schmid-Tannwald C, Kernt M, Kampik A, Neubauer AS. The NEI VFQ-25 vision-related quality of life and prevalence of eye disease in a working population. Graefes Arch Clin Exp Ophthalmol. 2010;248(1):85-92.
29. Stein JD, Newman-Casey PA, Mrinalini T, Lee PP, Hutton DW. Cost-effectiveness of bevacizumab and ranibizumab for newly diagnosed neovascular macular degeneration. Ophthalmology. 2014;121(4):936-45.

Funding: No specific financial support was available for this study
CEP Approval: Comitê de Ética em Pesquisa da Faculdade de Medicina, Universidade de São Paulo. Research protocol: 253/15. Date of approval: 24 June 2015
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
May 24, 2018.
Accepted on:
July 25, 2018.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket