

Luiza Carneiro Bertazzi1; Renan Carneiro Nogueira Bertazzi2; Aline Pimentel de Miranda1; Júlia Cristina Lima1; Juliana Ishii Iguma1; José Vital Filho1
DOI: 10.17545/eOftalmo/2026.v12.006
ABSTRACT
The aim of this report is to describe a rare case of melanoma metastatic to the orbit and to emphasize the clinical, imaging, histopathological, and therapeutic findings, as well as to contextualize these observations within a review of the recent literature. This case report includes the clinical presentation, ophthalmic evaluation, imaging studies, histopathology, and immunohistochemistry, along with an integrative discussion based on published evidence. A 66-year-old man presented with headache, eye pain, and progressive swelling of the left eye, which evolved to proptosis and spontaneous ocular bleeding. Computed tomography of the orbit showed diffuse thickening of the lateral and superior rectus muscles, with anteromedial displacement of the globe. Histopathology revealed pleomorphic tumor cells containing melanocytic pigment, and the diagnosis was confirmed by immunohistochemistry, which showed positivity for HMB-45, Melan-A, and S100, along with focal expression of CD56. Systemic staging identified hepatic and lung metastases, consistent with advanced disease and a poor prognosis. The patient was referred for palliative systemic oncologic treatment, highlighting the diagnostic challenges and therapeutic limitations often reported in the literature for this rare entity. Orbital melanoma, particularly in the metastatic context, is a rare and aggressive condition associated with an unfavorable prognosis. Diagnosis depends on a combination of clinical assessment, imaging studies, histopathology, and immunohistochemistry. This case reinforces the need for a multidisciplinary evaluation and highlights the importance of further research to optimize therapeutic strategies in this uncommon clinical scenario.
Keywords: Melanoma; Orbital neoplasms; Orbit; Histopathology; Immunohistochemistry.
RESUMO
O objetivo é descrever um caso raro de melanoma metastático com acometimento orbitário, enfatizando os achados clínicos, de imagem, histopatológicos e terapêuticos, além de contextualizar essas observações com uma revisão da literatura recente. Relato de caso incluindo apresentação clínica, avaliação oftalmológica, exames de imagem, histopatologia e imunohistoquímica, seguido de discussão integrativa com a evidência publicada. Um homem de 66 anos apresentou cefaleia, dor ocular e edema progressivo do olho esquerdo, que evoluiu para proptose e sangramento ocular espontâneo. A tomografia computadorizada de órbita revelou espessamento difuso dos músculos retos lateral e superior, com deslocamento anteromedial do globo. A histopatologia mostrou células tumorais pleomórficas com pigmento melanocítico, e a imunohistoquímica confirmou o diagnóstico por meio de positividade para HMB-45, Melan-A e S100, além de expressão focal de CD56. O estadiamento sistêmico identificou metástases hepáticas e pulmonares, compatíveis com doença avançada e prognóstico reservado. O paciente foi encaminhado para terapia oncológica sistêmica paliativa, destacando os desafios diagnósticos e as limitações terapêuticas frequentemente relatadas na literatura para essa entidade rara. O melanoma orbitário, especialmente no contexto metastático, é uma condição rara e agressiva, associada a prognóstico desfavorável. O diagnóstico depende da combinação entre avaliação clínica, exames de imagem, histopatologia e imunohistoquímica. Este caso reforça a necessidade de avaliação multidisciplinar e destaca a importância de pesquisas adicionais para otimizar estratégias terapêuticas nesse cenário clínico incomum.
Palavras-chave: Melanoma; Neoplasias orbitárias; Órbita; Histopatologia; Imunohistoquímica.
INTRODUCTION
Orbital melanoma is a rare malignant tumor that presents considerable diagnostic and therapeutic challenges. It can be classified as primary, when originating from ectopic melanocytes within the orbit, or secondary (metastatic), when resulting from the hematogenous spread of cutaneous, uveal, or conjunctival melanoma. Primary orbital melanoma accounts for less than 1% of all orbital tumors, whereas metastatic lesions are more common and usually indicate advanced systemic disease1,2.
Over the past decades, the global incidence of cutaneous melanoma has steadily increased, along with a growing number of orbital metastases. Most patients are adults in the fifth to seventh decades of life, and there is no clear predominance of either sex3,4. Large series describe secondary orbital melanoma as more prevalent than primary disease, typically reflecting disseminated systemic involvement5,6.
Clinically, orbital melanoma may present with rapidly progressive proptosis, eyelid swelling, diplopia, and orbital pain. However, these manifestations are nonspecific and can mimic other orbital masses, such as meningioma, lymphoma, or cavernous hemangioma, making the initial diagnosis challenging7,8. Diagnostic confirmation is based on histopathological evaluation combined with immunohistochemistry, with melanocytic markers such as S100, HMB-45, and Melan-A9,10 frequently expressed.
The prognosis of metastatic orbital melanoma is generally poor, with the liver being the most frequent site of metastasis, followed by the lungs and the central nervous system. Historical series have reported a median survival ranging from 6 to 12 months after the diagnosis of orbital metastasis5,11.
In this context, case reports remain important for illustrating uncommon clinical presentations and diagnostic and therapeutic challenges. Here, we describe a rare case of orbital melanoma and highlight the clinical, imaging, and histopathological findings, along with aspects related to disease management.
Recent systematic reviews and institutional cohorts have confirmed the exceptional rarity of orbital melanoma, noting that primary cases are uncommon and often associated with pre-existing melanocytic lesions, whereas secondary cases predominate2,6. Large retrospective series have shown that surgical excision remains the mainstay of local treatment, although complete resection is often limited by tumor extent and orbital anatomy7.
The therapeutic arsenal for advanced melanoma has expanded considerably over the last decade. In addition to checkpoint inhibitors and tebentafusp, several targeted agents and experimental strategies are under clinical evaluation, particularly for tumors exhibiting uncommon genetic alterations. Early clinical experience suggests that combining immunotherapy with targeted approaches may further enhance treatment efficacy and prolong survival in selected subgroups of patients with orbital involvement12-16.
Published series on orbital melanoma remain scarce, with most evidence derived from small retrospective cohorts and case reports1,2,6,7,10. These studies highlight the heterogeneity of clinical presentation, ranging from indolent lesions confined to the orbit to aggressive tumors with early systemic dissemination. Despite gradual therapeutic advances, the overall prognosis remains poor, underscoring the need for multicenter collaboration and long-term follow-up to better characterize prognostic determinants and optimize therapeutic strategies8,11,15.
Despite these advances, local recurrence and systemic progression remain common. Long-term follow-up data indicate that, even after radical surgery, overall survival remains unsatisfactory, emphasizing the need for early detection and individualized therapeutic approaches8,13,16. Collaborative studies and pooled analyses are essential to better define prognostic factors and refine management algorithms for this uncommon neoplasm.
CASE REPORT
A 66-year-old man was referred to the ophthalmology department with a 1-month history of progressively worsening left-sided headache and ocular pain, followed by eyelid swelling, proptosis, and subconjunctival bleeding. He denied smoking or alcohol consumption. His medical history included diabetes mellitus and hypertension. His ophthalmic history was notable for keratoconus, for which he had undergone penetrating keratoplasty in the right eye approximately 30 years earlier.
At the initial ophthalmic examination, best-corrected visual acuity was 1.3 logMAR in the right eye and 0.69 logMAR in the left eye. Hertel exophthalmometry revealed asymmetrical proptosis, measuring 18 mm in the right eye and 23 mm in the left eye, with a base of 97 mm. Color vision assessment using the Ishihara test was normal in the right eye (16/16) and markedly reduced in the left eye (3/16). Ocular motility was preserved in the right eye, whereas the left eye showed restricted movement in all directions of gaze. Biomicroscopic examination revealed corneal opacity related to previous hydrops in the right eye and subconjunctival hemorrhage in the left eye. Fundus examination could not be performed in the right eye due to media opacity and was unremarkable in the left eye.
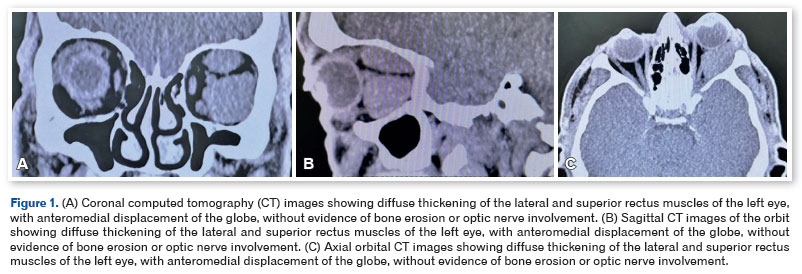
After referral to the Orbital Diseases Unit at Santa Casa de Misericórdia de São Paulo, temporary tarsorrhaphy was performed at the first consultation to protect the ocular surface. On admission, computed tomography (CT) of the orbits was performed in the Emergency Department and showed a diffuse infiltrative process involving the extraocular muscles, with thickening of the superior and lateral rectus muscles and anteromedial displacement of the left globe, resulting in proptosis (Figures 1A–C). The differential diagnosis included IgG4-related disease, orbital vascular disorders, lymphoproliferative disorders, and orbital metastasis.
In view of the initial suspicion of an orbital inflammatory process, empirical treatment with oral prednisone at 1 mg/kg/day was initiated; however, the patient's orbital pain and overall condition progressively worsened, with the development of dyspnea and marked weakness.
Approximately 5 weeks after symptom onset, given the patient's clinical deterioration, a lateral orbitotomy with diagnostic biopsy was performed. Intraoperatively, the lesion exhibited atypical pigmentation and friable tissue, suggestive of a melanocytic neoplasm.
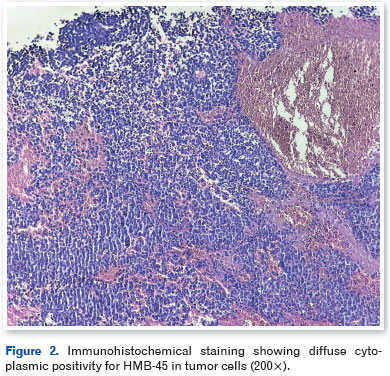
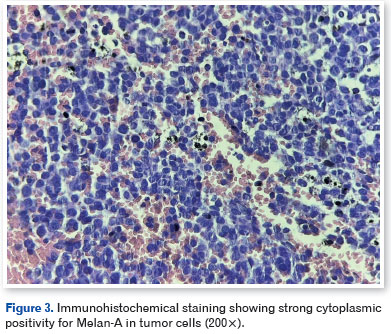
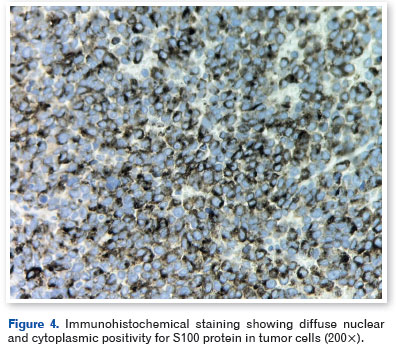
Histopathological examination revealed pleomorphic tumor cells containing melanocytic pigment. Immunohistochemistry showed diffuse positivity for HMB-45 (Figure 2), Melan-A (Figure 3), and S100 protein (Figure 4), along with focal expression of CD56. The tumor cells were negative for AE1/AE3, CD20, CD3, synaptophysin, and p63, consistent with a diagnosis of melanoma.
While awaiting definitive staging, the patient developed acute respiratory failure and rapid clinical deterioration. Systemic evaluation revealed multiple hepatic and pulmonary lesions with a metastatic pattern, consistent with disseminated disease. Despite supportive measures, the patient died during hospitalization before specific systemic oncologic treatment could be initiated.
In the absence of an identifiable primary lesion at presentation, the constellation of clinical, radiological, histopathological, and immunohistochemical findings was consistent with melanoma metastatic to the orbit from an occult primary site.
DISCUSSION
Orbital melanoma remains a rare clinical entity associated with high recurrence and mortality rates. Orbital metastatic involvement, although uncommon, reflects advanced disease progression and may even represent the first clinical manifestation of systemic dissemination1,2,5,6. Our patient presented with classic signs of orbital involvement, namely rapidly progressive proptosis, pain, and ocular bleeding, consistent with descriptions in the literature7,8.
Defining the primary site of the melanoma was challenging in this case. Unlike primary orbital melanomas, which are often associated with precursor lesions such as melanocytosis or blue nevi, and unlike secondary melanomas, which are usually linked to a prior history of cutaneous, uveal, or conjunctival melanoma, our patient had no history of cancer or identifiable cutaneous or ocular lesions. This challenge is not uncommon: in published series, the origin of up to 10%–15% of orbital melanoma cases remains undefined even after systemic investigation1,2,6.
The lack of molecular analysis was a significant limitation in this case. Evaluation of genetic alterations—such as mutations in GNAQ and GNA11, which are highly prevalent in uveal melanoma, and mutations in BAP1, SF3B1, and EIF1AX, which carry prognostic significance—could have enabled more robust classification. Limited access to these resources highlights ongoing barriers in many centers and does not detract from the clinical and scientific relevance of this report, which exemplifies the complexity of real-world cases9,11.
Exenteration remains a standard surgical approach for extensive primary cases; however, its role in metastatic disease is controversial, as it has not been shown to confer a survival advantage. Conservative orbitotomy may be considered for localized tumors, while endoscopic approaches are gaining acceptance in selected benign and malignant cases6,7,15. Nevertheless, surgery has a limited and predominantly palliative role in orbital metastatic melanoma5,10.
Radiotherapy may be considered in cases of local recurrence or positive margins. In uveal melanoma, brachytherapy and external beam radiotherapy can provide local control but are associated with significant ocular morbidity. In orbital melanoma, available evidence is limited and largely extrapolated from other anatomical sites8,9,16.
Recent advances in systemic therapy have reshaped the treatment landscape for melanoma. Immune checkpoint inhibitors (nivolumab, pembrolizumab, and ipilimumab) have improved survival in metastatic cutaneous melanoma12. BRAF/MEK-targeted therapies (dabrafenib/trametinib and vemurafenib/cobimetinib) offer additional benefits in selected patients14,16. In uveal melanoma, tebentafusp—an ImmTAC (monoclonal T-cell receptor designed to redirect the immune system against cancer)—demonstrated an overall survival benefit in a phase III clinical trial published in 2021, representing a significant advance for this subtype13. However, evidence regarding benefits specifically for orbital disease remains limited to case reports and small series1,6,10.
Although orbital melanoma is extremely rare, population studies indicate a steady global increase in melanoma incidence, which may indirectly contribute to more frequent detection of orbital metastases3,4. Overall prognosis remains poor, with the liver, lungs, and central nervous system being the most common metastatic sites5,11. Even in contemporary cohorts, survival following the diagnosis of orbital metastasis rarely exceeds 12 months, highlighting the aggressive nature of this presentation8,11.
Radiological assessment plays a key role in differentiating orbital melanoma from other benign and malignant orbital masses. CT and magnetic resonance imaging typically show infiltrative lesions involving extraocular muscles or orbital fat; however, these findings are not pathognomonic7,8. Therefore, immunohistochemistry remains essential, as the expression of melanocytic markers (S100, HMB-45, and Melan-A) is consistently reported, reinforcing their diagnostic reliability in clinical practice9,10.
In addition to checkpoint inhibition, ongoing research is exploring combinations of systemic therapies and their integration with locoregional treatments. For example, clinical experience with tebentafusp in uveal melanoma provides proof of concept that immune cell redirection strategies can improve survival even in historically refractory settings13. Although extrapolation to orbital melanoma remains speculative, these advances may lead to improved outcomes in the future12-14.
Given the rarity of orbital melanoma, most available evidence derives from isolated case reports and small institutional series1,2,6,10. These studies provide valuable insights into diagnostic challenges, therapeutic decision-making, and real-world outcomes. The present case adds to this body of knowledge by emphasizing the importance of early clinical suspicion, the diagnostic value of immunohistochemistry, and the persistent challenges in accessing molecular testing across many cancer centers worldwide9,11,16.
This case reinforces the importance of including melanoma in the differential diagnosis of rapidly progressive orbital masses and highlights ongoing diagnostic challenges related to the limited availability of molecular testing. Sharing such experiences enriches the collective understanding of this rare condition and supports further research into improved diagnostic and therapeutic strategies. These findings are consistent with previously published case series1,2,5,6.
In conclusion, orbital melanoma, whether primary or metastatic, remains a significant diagnostic and therapeutic challenge. Definitive diagnosis relies on histopathology and immunohistochemistry. Although surgery and radiotherapy may be considered in selected cases, patients with disseminated disease typically require palliative systemic management. Emerging strategies—including immunotherapy and molecularly targeted therapies—have shown promising results; however, evidence specific to orbital involvement remains limited. This case underscores the importance of multidisciplinary evaluation and highlights the need for further studies to refine management strategies and improve outcomes in this uncommon disease.
REFERENCES
1. Adetunji MO, McGeehan B, Lee V, Maguire MG, Briceño CA. Primary orbital melanoma: a report of a case and comprehensive review of the literature. Orbit. 2021;40(6):461-469.
2. Rose AM, Luthert PJ, Jayasena CN, Verity DH, Rose GE. Primary orbital melanoma: presentation, treatment, and long-term outcomes for 13 patients. Front Oncol. 2017 Dec 18:7:316.
3. Garbe C, Amaral T, Peris K, Hauschild A, Arenberger P, Basset-Seguin N, Bastholt L, Bataille V, Brochez L, Del Marmol V, Dréno B, Eggermont AMM, Fargnoli MC, Forsea AM, Höller C, Kaufmann R, Kelleners-Smeets N, Lallas A, Lebbé C, Leiter U, Longo C, Malvehy J, Moreno-Ramirez D, Nathan P, Pellacani G, Saiag P, Stockfleth E, Stratigos AJ, Van Akkooi ACJ, Vieira R, Zalaudek I, Lorigan P, Mandala M, European Association of Dermato-Oncology (EADO), the European Dermatology Forum (EDF), and the European Organization for Research and Treatment of Cancer (EORTC). European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment – Update 2024. Eur J Cancer. 2025 Jan 17:215:115153.
4. Butt K, Hussain R, Coupland S, Krishna Y. Conjunctival melanoma: a clinical review and update. Cancers (Basel). 2024; 16(18):3121.
5. Liarikos S, Rapidis AD, Roumeliotis A, Angelopoulos AP. Secondary orbital melanomas: analysis of 15 cases. J Craniomaxillofac Surg. 2000;28(3):148-52.
6. Figueira E, Rajak S, McKelvie P, Kalantzis G, Ismail A, Gonzales M, et al. Primary orbital melanoma: a case series and literature review. Orbit. 2018;37(5):352-357.
7. Reyes-Soto G, Carrillo-Hernández JF, Cacho-Díaz B, Ovalle CS, Castillo-Rangel C, Nurmukhametov R, et al. Surgical treatment of orbital tumors in a single center: analysis and results. Surg Neurol Int. 2024 Apr 5:15:122.
8. Huang YY, Hou TY, Yu WK, Tsai CC, Kao SC, Hsu WM, et al. The clinical feature and treatment outcome of ocular melanoma: a 34-year experience in a tertiary referral center. Cancers (Basel). 2021;13(23):5865.
9. Branisteanu DC, Bogdanici CM, Branisteanu DE, Maranduca MA, Zemba M, Balta F, et al. Uveal melanoma diagnosis and current treatment options (Review). Exp Ther Med. 2021;22(6):1428.
10. Ferreira AF, Silveira Filho LG, Dias EL. Primary orbital melanoma in an anophthalmic socket. Radiol Bras. 2019;52(5):347-348.
11. Liu X, Yue H, Jiang S, Kong L, Xu Y, Chen Y, et al. Clinical features and prognosis of patients with metastatic ocular and orbital melanoma: a bi-institutional study. Cancer Med. 2023;12(15): 16163-16172.
12. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019; 381(16):1535-1546.
13. Nathan P, Hassel JC, Rutkowski P, Baurain JF, Butler MO, Schlaak M, Sullivan RJ, Ochsenreither S, Dummer R, Kirkwood JM, Joshua AM, Sacco JJ, Shoushtari AN, Orloff M, Piulats JM, Milhem M, Salama AKS, Curti B, Demidov L, Gastaud L, Mauch C, Yushak M, Cavajal RD, Hamid O, Abdullah SE, Holland C, Goodall H, Piperno-Neumann S.; IMCgp100-202 Investigators. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N Engl J Med. 2021;385(13):1196-1206.
14. Knight A, Karapetyan L, Kirkwood JM. Immunotherapy in melanoma: recent advances and future directions. Cancers (Basel). 2023;15(4):1106.
15. Lehmann AE, von Sneidern M, Shen SA, Humphreys IM, Abuzeid WM, Jafari A. Does reconstruction affect outcomes following exclusively endoscopic endonasal resection of benign orbital tumors: a systematic review with meta-analysis. World J Otorhinolaryngol Head Neck Surg. 2022;8(1):25-35.
16. Lens MB, Eisen TG. Systemic chemotherapy in the treatment of malignant melanoma. Expert Opin Pharmacother. 2003; 4(12):2205-11.
| AUTHOR INFORMATION |
|
 |
» Luiza Carneiro Bertazzi http://orcid.org/0009-0002-1373-2780 http://lattes.cnpq.br/7468696785742243 |
 |
» Aline Pimentel de Miranda http://orcid.org/0000-0002-3017-7005 https://lattes.cnpq.br/1135148626230448 |
 |
» Renan Carneiro Nogueira Bertazzi http://orcid.org/0009-0003-9606-1368 http://lattes.cnpq.br/3035187367135853 |
 |
» Júlia Cristina Lima http://orcid.org/0009-0008-4661-5509 https://lattes.cnpq.br/1104522340146177 |
 |
» Juliana Ishii Iguma http://orcid.org/0000-0002-8745-6582 https://lattes.cnpq.br/9614009693321638 |
 |
» José Vital Filho http://orcid.org/0000-0002-1669-0398 https://lattes.cnpq.br/2460766132336890 |
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
December 1, 2025.
Accepted on:
March 18, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket