

Glauco Batista Almeida
DOI: 10.17545/eOftalmo/2026.0003
Este artigo pertence à Edição Especial SLT no Glaucoma: Da Prática Clínica à Perspectiva de Implementação no SUS
ABSTRACT
Glaucoma is a chronic and progressive disease, and reduction of intraocular pressure remains the only confirmed strategy for slowing the progression of optic nerve damage. Traditionally, initial treatment is based on the continuous use of hypotensive eye drops; however, this approach relies heavily on patient compliance and is associated with adverse effects, namely on the ocular surface, and thus, ultimately impairing the quality of life. Considering this background, selective laser trabeculoplasty has emerged as an effective and safe alternative and does not require daily medication use. Current evidence, especially from the LiGHT multicenter randomized clinical trial, indicates that selective laser trabeculoplasty has a sustained hypotensive efficacy comparable to treatment with medications while being associated with less treatment intensification, less disease progression, and less demand for filtering surgery during follow-up. Although the overall quality of life scores are similar between the two strategies, initiating treatment with selective laser trabeculoplasty is associated with a lower treatment burden, greater autonomy, and greater patient satisfaction. Despite the solid scientific basis, the use of selective laser trabeculoplasty is limited due to challenges in training of ophthalmologists, doctor–patient communication, and availability of equipment. Thus, the choice between selective laser trabeculoplasty and eye drops must address efficacy, compliance, and quality of life using an individualized and patient-centered approach.
Keywords: Selective laser trabelucoplasty; Adherence to treatment; Quality of life.
RESUMO
O glaucoma é uma doença crônica e progressiva, na qual a redução da pressão intraocular (PIO) permanece como a única estratégia comprovadamente eficaz para retardar a progressão do dano ao nervo óptico. Tradicionalmente, o tratamento inicial baseia-se no uso contínuo de colírios hipotensores; contudo, essa abordagem depende fortemente da adesão do paciente e está associada a efeitos adversos, impacto sobre a superfície ocular e prejuízo à qualidade de vida. Nesse contexto, a trabeculoplastia seletiva a laser (SLT) surge como uma alternativa eficaz e segura, independente do uso diário de medicações. Evidências contemporâneas, especialmente do ensaio clínico randomizado multicêntrico LiGHT, demonstram que a trabeculoplastia seletiva a laser apresenta eficácia hipotensora sustentada comparável ao tratamento medicamentoso, com menor necessidade de intensificação terapêutica, menor progressão da doença e menor demanda por cirurgias filtrantes ao longo do seguimento. Embora os escores globais de qualidade de vida sejam semelhantes entre as estratégias, o tratamento inicial com trabeculoplastia seletiva a laser associa-se a menor carga terapêutica, maior autonomia e maior satisfação do paciente. Apesar do sólido embasamento científico, a adoção do trabeculoplastia seletiva a laser ainda enfrenta barreiras relacionadas à formação do oftalmologista, à comunicação médico-paciente e à disponibilidade do equipamento. Assim, a escolha entre trabeculoplastia seletiva a laser e colírios deve integrar eficácia, adesão e qualidade de vida, dentro de uma abordagem individualizada e centrada no paciente.
Palavras-chave: Trabelucoplastia seletiva a laser; Adesão ao tratamento; Qualidade de vida.
INTRODUCTION
Glaucoma is a chronic and progressive disease characterized by damage to the optic nerve and irreversible visual loss, and reducing intraocular pressure (IOP) is the only effective strategy know to slow its progression. Traditionally, the initial treatment is based on the continuous use of hypotensive eye drops, which have well-established efficacy in reducing IOP. However, this approach is highly dependent on patient adherence to daily treatment, a particularly challenging aspect in a disease that is often asymptomatic and has a slow progression and high functional morbidity1,2.
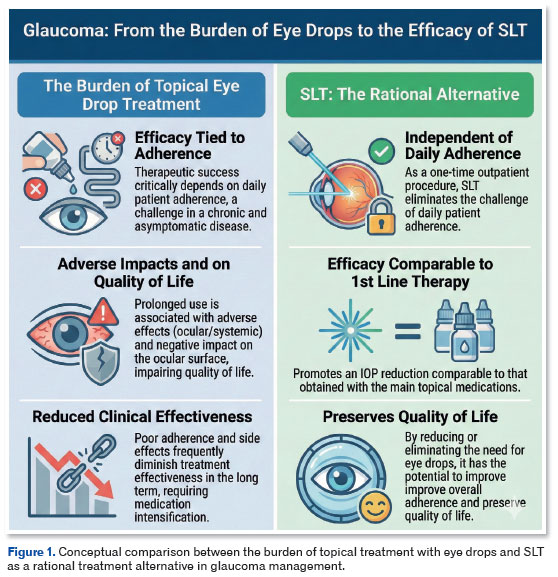
Despite the pharmacological efficacy demonstrated in clinical trials, prolonged use of eye drops is associated with significant rates of low treatment adherence, ocular and systemic adverse effects, a negative impact on the ocular surface, and impaired quality of life. These factors often reduce the long-term clinical effectiveness of treatment, leading to frequent treatment adjustments, intensification of drug treatment, and increased treatment burden for the patient and the healthcare system3,4.
In this regard, selective laser trabeculoplasty (SLT) has emerged as an effective alternative to topical treatment, and SLT promotes an IOP reduction similar to first-line medications through a single outpatient procedure that is safe and does not require daily adherence. By reducing or eliminating the need for eye drops, SLT has the potential to improve overall adherence to treatment and preserve health-related quality of life. Thus, the comparison between SLT and eye drops is important not only for the magnitude of the pressure reduction but also for its functional, behavioral, and patient-centered effects (Figure 1)3,5-7.
In addition to discussing efficacy, adherence, and quality of life, this chapter highlights the potential barriers for ophthalmologists in relation to SLT and the patients’ perspective of this treatment.
SLT versus eye drops in the treatment of glaucoma: current evidence on sustained efficacy, adherence, and quality of life
The LiGHT multicenter randomized clinical trial compared SLT with topical drug treatment as initial treatment for patients with ocular hypertension and open-angle glaucoma, using a treatment protocol guided by individualized pressure targets according to disease severity. Treatment efficacy was mainly assessed by the ability to maintain IOP within the target over time, with therapeutic escalation if needed7.
After 36 months of follow-up, pressure values were similar between the two groups. The final mean IOP was 16.6 mmHg in the SLT group and 16.3 mmHg in the eye drops group, with no clinically relevant difference. Moreover, the proportion of eyes with IOP within target was high in both arms (95.0% in SLT vs. 93.1% in eye drops), as was the proportion of visits in which IOP values were on target throughout the follow-up (93.0% vs. 91.3%, respectively). These findings demonstrate that over a 3-year period, the hypotensive efficacy of SLT as initial treatment was not inferior to that of drug treatment7.
A distinct aspect observed at 3 years was the lower need for additional treatment in the SLT group. Approximately 78% of the patients initially treated with SLT did not require eye drops and their pressure remained adequately controlled, whereas the group initially treated with medication showed a greater need for treatment intensification over time7.
In the extension of the study to 72 months, which allowed crossover between the groups after the third year, the overall rates of patients with controlled pressure remained high and were similar between the groups. At 6 years, the mean IOP was slightly lower in the group initially treated with eye drops (15.4 mmHg) than in the group initially treated with SLT (16.3 mmHg). However, this difference occurred in a context of a higher number of treatment intensifications and surgical procedures in the eye drops group over the course of the follow-up8.
Despite the slightly lower final IOP in the drug group, the group initially treated with SLT showed less disease progression and less need for filtering surgery over the 6 years. Additionally, the pressure was on target in approximately 70% of the eyes initially treated with SLT, without the use of eye drops or incisional surgery, in contrast to approximately 18% in the group initially treated with medication. These data confirm that the efficacy of SLT should be interpreted not only according to the final IOP alone but also according the behavior of pressure over time8.
When analyzed by severity, the results at 3 years showed similar pressure control between SLT and eye drops in cases of mild and moderate glaucoma, with target rates consistently higher than 94% of eyes in both groups. In more severe cases, although the proportion of eyes on target was lower, there was no relevant difference between the initial strategies, which indicates similar hypotensive efficacy within the limits of the study design. However, patients with advanced glaucoma tend to require lower pressure targets and show less tolerance to fluctuations, often requiring combined treatments or surgery.
In the LiGHT study, health-related quality of life was similar between the SLT and eye drops arms after 3 and 6 years of follow-up. However, initial treatment with SLT allowed maintaining quality of life with a lower treatment load, being less dependent on topical medications, and suffering less cumulative exposure to adverse effects. This suggests that the main advantage of SLT lies in better adherence to treatment and preservation of quality of life over time rather than in differences in traditional global scores.
From the clinical trial to the physician’s office: why is SLT still not widely indicated by ophthalmologists?
An important barrier for ophthalmologists in relation to SLT is the lack of information about the procedure.
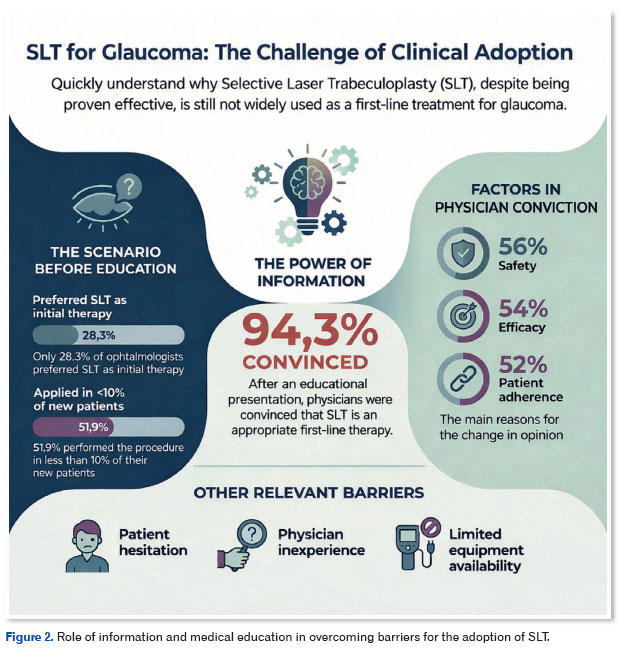
Before the educational intervention, 84.9% of the participants reported proposing laser treatment to newly diagnosed patients but only 28.3% preferred it as first-line treatment over medication (67.9%). Moreover, 47.2% of physicians considered SLT to be a first-line treatment, whereas 35.8% considered it to be a second-line treatment. However, 51.9% of physicians reported that 0%–10% of their patients with newly diagnosed primary open-angle glaucoma actually received SLT. After attending the educational presentation, 94.3% of the participants reported being convinced that SLT is an appropriate first-line treatment for open-angle glaucoma. The main reasons given for this belief were safety (56.0%), efficacy (54.0%), and adherence (52.0%).
Other important reasons for the limited use of the laser treatment are patient hesitation, physician’s inexperience, and limited availability of the device9.
Thus, the expansion of the use of SLT in clinical practice depends fundamentally on: strengthening the training of ophthalmologists (especially of general ophthalmologists), including training in communicating clearly and in a balanced way with patients about the advantages and limitations of the procedure, gaining practical experience with the technique, and increasing the availability of the equipment in both public and private networks (Figure 2).
Patient’s perspective: how SLT is perceived in the glaucoma treatment experience
In the LiGHT study, health-related quality of life was similar between the SLT and eye drops arms after 3–6 years of follow-up. The study by De Keyser et al. showed less need for help with using eye drops at 6 months (9.38% vs. 31.15% in the control group, p = 0.002) and at 12 months (12.24% vs. 36.67% in the control group, p = 0.01). The patients also showed significant improvements in terms of quality of life and satisfaction with the treatment in relation to the following parameters (at 12 months)10:
- Perceived Efficacy: Increased confidence in the treatment (SLT: 65.79 to 77.99, p < 0.001).
- Side Effects: Fewer complaints about side effects (SLT: 67.51 to 75.00, p = 0.006).
- Eye Appearance: Fewer complaints about changes in eye appearance (SLT: 74.93 to 83.93, p = 0.003).
- Convenience of Use: Less hassle with eye drops (SLT: 67.56 to 83.38, p < 0.001).
Key takeaway
Comparison between SLT and eye drops for the treatment of glaucoma shows that treatment efficacy should not be assessed by the reduction in intraocular pressure alone but also by the ability to maintain control of the disease over time, with good adherence and preservation of quality of life. Available evidence shows that SLT has sustained hypotensive efficacy, with less dependence on topical medication and a lower treatment burden for the patient.
Despite this solid scientific basis for using SLT, the adoption of this treatment still faces challenges related to the training of ophthalmologists, doctor–patient communication, and structural availability. However, from the patient’s perspective, SLT is an alternative treatment that improves autonomy, convenience, and overall satisfaction.
Thus, the choice between SLT and eye drops must take into consideration the scientific evidence, clinical context, and patient preference, as well as the need for an individualized therapeutic approach focused on long-term effectiveness in the management of glaucoma.
REFERENCES
1. Haymes SA, LeBlanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Risk of Falls and Motor Vehicle Collisions in Glaucoma. Investig Opthalmol Vis Sci. 2007;48(3):1149-55.
2. Garway-Heath DF, Crabb DP, Bunce C, Lascaratos G, Amalfitano F, Anand N, et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;385(9975):1295-304.
3. Lee R, Hutnik CML. Projected cost comparison of selective laser trabeculoplasty versus glaucoma medication in the Ontario Health Insurance Plan. Can J Ophthalmol J Can d’Ophtalmol. 2006;41(4):449-56.
4. Kirwan JF, Nightingale JA, Bunce C, Wormald R. Beta blockers for glaucoma and excess risk of airways obstruction: population based cohort study. BMJ. 2002;325(7377):1396-7.
5. Medeiros FA, Gracitelli CPB, Boer ER, Weinreb RN, Zangwill LM, Rosen PN. Longitudinal Changes in Quality of Life and Rates of Progressive Visual Field Loss in Glaucoma Patients. Ophthalmology. 2015;122(2):293-301.
6. Nordmann J-P, Auzanneau N, Ricard S, Berdeaux G. Vision related quality of life and topical glaucoma treatment side effects. Heal Qual Life Outcomes. 2003 Dec 10:1:75.
7. Gazzard G, Konstantakopoulou E, Garway-Heath D, Garg A, Vickerstaff V, Hunter R, Ambler G, Bunce C, Wormald R, Nathwani N, Barton K, Rubin G, Buszewicz M; LiGHT Trial Study Group. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505-1516.
8. Gazzard G, Konstantakopoulou E, Garway-Heath D, Adeleke M, Vickerstaff V, Ambler G, Hunter R, Bunce C, Nathwani N, Barton K; LiGHT Trial Study Group. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial Six-Year Results of Primary Selective Laser Trabeculoplasty versus Eye Drops for the Treatment of Glaucoma and Ocular Hypertension. Ophthalmology. 2023;130(2):139-151.
9. Bonafede L, Sanvicente CT, Hark LA, Tran J, Tran E, Zhang Q, et al. Beliefs and Attitudes of Ophthalmologists Regarding SLT as First Line Therapy for Glaucoma. J Glaucoma. 2020;29(10): 851-856.
10. De Keyser M, De Belder M, De Groot V. Quality of life in glaucoma patients after selective laser trabeculoplasty. Int J Ophthalmol. 2017;10(5):742-748.
| INFORMAÇÕES DOS AUTORES |
|
 |
» Glauco Batista Almeida http://lattes.cnpq.br/2117165254457635 https://orcid.org/0000-0002-0036-1223 |
Funding: The author declare no funding.
Conflicts of interest: The author declare no funding.
Received on:
January 14, 2025.
Accepted on:
January 29, 2025.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket