

Isabella Passarelli Giabardo Marques; Caio Henrique Peres Oliani; Guilherme de Oliveira Aurich; Guilherme Lopes Coelho, Marcello Novoa Colombo Barboza, Priscilla Fernandes Nogueira
DOI: 10.17545/eOftalmo/2024.0030
ABSTRACT
OBJECTIVES: To describe the epidemiological profile and clinical manifestations of direct carotid-cavernous fistulas in elderly patients through two case reports.
METHODS: This was a retrospective descriptive study involving two patients treated at Laser Vision Hospital in Brazil. Both underwent complete ophthalmologic examinations and magnetic resonance angiography (MRA).
RESULTS: Case 1: A 78-year-old hypertensive female patient presented with sudden onset of severe eye pain, proptosis, chemosis, diffuse conjunctival hyperemia, complete ophthalmoplegia, orbital bruit, and tinnitus on the right side. Magnetic resonance angiography confirmed the presence of a direct carotid-cavernous fistula. The patient underwent endovascular treatment, with complete resolution of the condition. Case 2: A 69-year-old female patient reported recently onset binocular diplopia accompanied by mild proptosis. The clinical signs were suggestive of Dandy’s triad (chemosis, proptosis, and orbital bruit) and isolated paralysis of the sixth cranial nerve (abducens nerve). Magnetic resonance angiography demonstrated a direct carotid-cavernous fistula. The patient is currently under follow-up and awaiting endovascular treatment. These two cases illustrate different degrees of clinical involvement and reflect the variability in the presentation of direct carotid-cavernous fistulas.
CONCLUSIONS: Although direct carotid-cavernous fistulas are commonly associated with trauma, they may occur spontaneously in elderly patients due to vascular fragility. They are characterized by sudden onset and prominent orbital manifestations such as proptosis, conjunctival hyperemia, and ophthalmoplegia. Early diagnosis and timely endovascular treatment are essential for preserving visual and neurological function.
Keywords: Carotid-cavernous fistula; Vision disorders; Abducens nerve palsy; Magnetic resonance angiography; Therapeutic embolization.
RESUMO
OBJETIVOS: Descrever o perfil epidemiológico e as manifestações clínicas de fístulas carótido-cavernosas (FCC) diretas em pacientes idosos, por meio de dois relatos de caso.
MÉTODOS: Estudo descritivo retrospectivo envolvendo dois pacientes atendidos no Hospital Visão Laser, Brasil. Ambos foram submetidos a exame oftalmológico completo e angio ressonância magnética. O estudo foi aprovado pelo comitê de ética em pesquisa (Plataforma Brasil – CAAE: 76124923.3.0000.0175), e todos os participantes assinaram o termo de consentimento livre e esclarecido.
RESULTADOS: Caso 1: Paciente do sexo feminino, 78 anos, hipertensa, apresentou início súbito de dor ocular intensa, proptose, quemose, hiperemia conjuntival difusa, oftalmoplegia completa, sopro orbitário e zumbido à direita. A angiorressonância confirmou a presença de FCC direta. A paciente foi submetida a tratamento endovascular com resolução completa do quadro. Caso 2: Paciente do sexo feminino, 69 anos, referiu diplopia binocular de início recente, acompanhada de proptose discreta, sinais clínicos compatíveis com a tríade de Dandy (quemose, proptose e sopro orbitário) e paralisia isolada do sexto nervo craniano (nervo abducente). A angio ressonância revelou FCC direta, e a paciente encontra-se em acompanhamento, aguardando tratamento endovascular. Os dois casos ilustram diferentes graus de comprometimento clínico, refletindo a variabilidade na apresentação das FCCs diretas.
CONCLUSÕES: As fístulas carótido-cavernosas diretas, embora comumente associadas a trauma, podem ocorrer espontaneamente em idosos devido à fragilidade vascular. São caracterizadas por início abrupto e manifestações orbitárias evidentes, como proptose, hiperemia conjuntival e oftalmoplegia. O reconhecimento precoce e o tratamento endovascular oportuno são fundamentais para preservar a função visual e neurológica.
Palavras-chave: Fístula carótido-cavernosa; Distúrbios da visão; Paralisia do nervo abducente; Angiorressonância magnética; Embolização terapêutica.
INTRODUCTION
A carotid-cavernous fistula (CCF) is a pathological communication between the internal carotid artery (ICA) and the cavernous sinus. The Barrow et al. classification divides CCFs into four types: type A is a direct high-flow fistula involving a rupture of the ICA into the cavernous sinus, while types B, C, and D are indirect low-flow fistulas, usually involving dural branches of the internal or external carotid arteries1.
Direct CCFs are most often associated with head trauma and represent the most severe and symptomatic form, with symptoms developing rapidly. Although they occur more commonly in young men following trauma, they may also occur spontaneously in the elderly, usually related to aneurysmal rupture of the intracavernous ICA or vascular fragility due to hypertension and atherosclerosis2,3.
Clinically, direct CCFs cause an abrupt rise in orbital venous pressure, resulting in proptosis, chemosis, conjunctival congestion, pulsatile bruits, and paralysis of the III, IV, and VI cranial nerves. Dandy’s triad (proptosis, orbital bruit, and conjunctival congestion) is highly suggestive4. Digital cerebral angiography is the gold-standard diagnostic examination; however, other imaging tests, such as magnetic resonance angiography (MRA), may demonstrate dilation of the superior ophthalmic vein and alterations in the cavernous sinus5.
Treatment is primarily endovascular, with high rates of fistula occlusion and significant clinical improvement. A multidisciplinary approach involving ophthalmologists, neuroradiologists, and neurosurgeons is essential6.
METHODS
This was a descriptive retrospective case report involving two patients treated at Laser Vision Hospital. Both underwent clinical evaluation with complete ophthalmologic examination and imaging studies. The study was approved by the Research Ethics Committee (Plataforma Brasil – CAAE: 76124923.3.0000.0175), in accordance with the Declaration of Helsinki and CNS Resolution 466/2012. The patients signed informed consent forms for the publication of their clinical data and case images. Data were extracted from medical records and analyzed descriptively, with emphasis on clinical and imaging findings and the management approach used in each case.
RESULTS
Case 1
A 78-year-old Caucasian woman with a history of systemic arterial hypertension presented to the ophthalmology department complaining of pain, redness, and blepharoptosis in her right eye (OD) for the past 10 days. She reported severe headache associated with tinnitus, more pronounced in the right ear. She denied any history of trauma or previous surgery. An anterior cranial CT scan was considered normal.
On ophthalmologic examination, the best-corrected visual acuity (BCVA) was 20/50 in both eyes (OU). External inspection of the OD revealed eyelid edema, ptosis, ecchymosis, and palpable fremitus (Figure 1A–B). Hertel exophthalmometry measurements were 24 mm in the OD and 18 mm in the left eye (OS), confirming right-sided proptosis.

Biomicroscopy of the OD showed marked chemosis (Figure 1C), grade 3 conjunctival hyperemia, dilated episcleral vessels, inferior band keratopathy, a deep anterior chamber, and stage 2–3 nuclear cataract. The OS was normal. Ocular motility showed complete ophthalmoplegia in the OD, while movements were preserved in the OS. Pupillary reflexes were present and symmetrical (3+) OU. Intraocular pressure (IOP) was 20 mmHg in OD and 16 mmHg in OS. Retinal mapping showed no alterations.
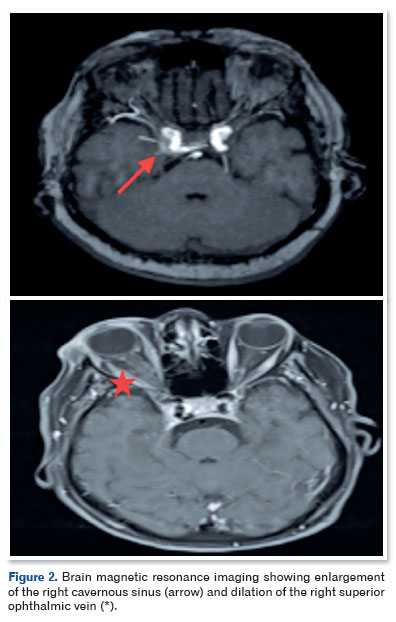
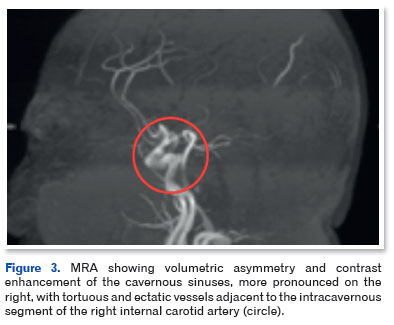
Cranial magnetic resonance imaging (Figure 2) and MRA (Figure 3) showed sinuous and ectatic vascular structures adjacent to the posteromedial wall of the intracavernous segment of the right ICA, as well as asymmetric dilation of the ipsilateral superior ophthalmic vein and grade II proptosis. These findings were consistent with the diagnosis of a direct CCF.
The patient was referred for neurosurgical evaluation and underwent successful endovascular treatment. Two months after embolization, she returned for ophthalmological follow-up with complete resolution of the clinical signs. BCVA remained 20/50 OU. Biomicroscopy showed no hyperemia, transparent corneas, and deep anterior chambers OU. Ocular motility was fully restored, fremitus was absent, and the patient was asymptomatic and pain-free.
Case 2
A 69-year-old woman presented to the ophthalmology emergency department complaining of binocular diplopia and redness in the OS that began the previous day. She reported headache and tinnitus in her left ear for about 1 month. She had no history of ophthalmologic disease or systemic comorbidities.
Examination showed an off-center Hirschberg reflex, and the prism cover test demonstrated 20 prism diopters of esotropia at distance. Duction and version testing revealed hypofunction of the left lateral rectus muscle (grade +3), consistent with abducens nerve palsy (Figure 4). BCVA was 20/25 in OU. Ectoscopy revealed proptosis of the OS with palpable fremitus. Hertel exophthalmometry measurements were 17 mm in OD and 20 mm in OS, with >2 mm asymmetry indicating proptosis.
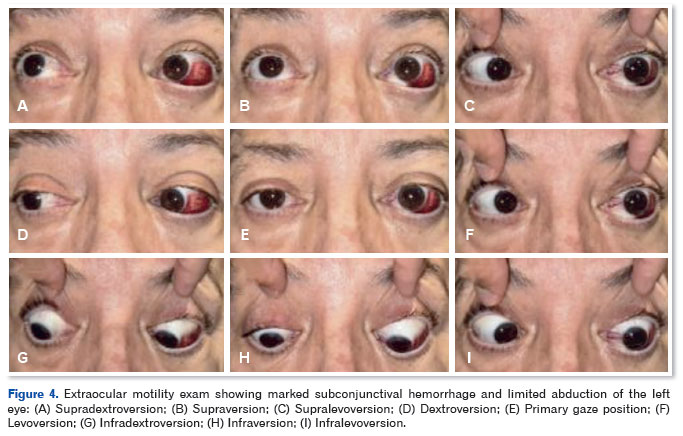
Biomicroscopy showed dilated nasal conjunctival vessels and subconjunctival hemorrhage in the temporal and inferior quadrants. Fundus examination revealed a pink optic disc with well-defined margins and a cup-to-disc ratio of 0.2 OU, with no abnormalities in the posterior pole. IOP was 14 mmHg OU.
The clinical presentation included classic Dandy’s triad—pulsatile proptosis, orbital bruit, and conjunctival hyperemia—strongly suggestive of a direct CCF associated with sixth nerve palsy.
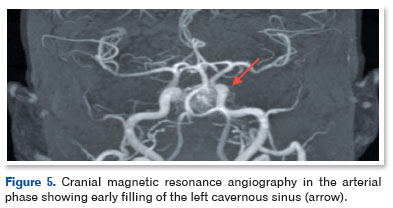
The patient was referred for neurological assessment. Arterial and venous MRA of the brain and cervical vessels demonstrated vascular prominence in the left cavernous sinus, adjacent to the cavernous segment of the ipsilateral ICA, as well as signs of venous congestion at the skull base (Figure 5). These findings were consistent with a direct left-sided CCF.
The patient remains under follow-up and is awaiting additional testing for endovascular treatment planning.
DISCUSSION
The cases presented illustrate the clinical manifestations of CCF in elderly patients and highlight the phenotypic variability and potential severity of these arteriovenous communications. Typically, direct CCFs are more frequent in young adult males following head trauma, accounting for up to 75% of cases described in some series2,3. However, there are increasing reports of spontaneous presentations in the elderly, usually associated with rupture of cavernous aneurysms or fragility of the intracavernous ICA wall due to systemic arterial hypertension, atherosclerosis, and microangiopathy2,6. Our two cases reinforce that patient age does not exclude the possibility of a direct CCF and that clinical vigilance is required even in the absence of trauma.
The pathophysiology of a direct CCF involves rupture of the ICA wall, creating a high-flow communication with the cavernous sinus. High-pressure arterial flow is diverted into the cavernous venous system, producing acute orbital venous hypertension. This results in proptosis, chemosis, dilation of episcleral vessels, diffuse conjunctival hyperemia, and, in more severe cases, oculomotor paralysis due to compression of cranial nerves III, IV, and VI within the cavernous sinus7. The pulsatile orbital bruit, often audible on examination, is among the most specific signs and was present in both reported cases.
Patient 1 exhibited a more exuberant presentation, with complete ophthalmoplegia, severe chemosis, and ocular pain, findings typical of a high-flow fistula. Patient 2, in contrast, presented with classic Dandy’s triad and isolated sixth nerve palsy, a common feature because the abducens nerve is the most vulnerable structure within the cavernous sinus. This contrast demonstrates how the caliber of the arterial rupture, shunt volume, and venous drainage pathways influence clinical severity8.
The course of direct CCFs is usually acute and rapidly progressive, unlike indirect forms, which develop more insidiously. While the abrupt onset often facilitates clinical suspicion, it also increases the risk of complications if treatment is delayed. Reported complications include ischemic optic neuropathy, secondary glaucoma from elevated episcleral venous pressure, retinal embolism, and even intracranial hemorrhage7,9. Therefore, early recognition of sudden orbital signs, especially in elderly patients reporting pulsatile bruits, is essential to reduce the risk of irreversible sequelae.
Digital subtraction angiography remains the gold standard because it allows detailed characterization of the fistula anatomy and guides therapeutic planning. However, MRA, which was used in our cases, has proved to be a valuable tool as an initial exam because it shows dilatation of the superior ophthalmic vein, changes in the cavernous sinus, and patterns of orbital venous congestion. These findings are highly suggestive of direct CCF and justify prompt subsequent invasive investigation5,6.
Endovascular treatment is the current therapeutic standard, with occlusion rates exceeding 90% in large series6,9. The choice of technique—transarterial, transvenous, or hybrid embolization—depends on the individual anatomy of the fistula and vascular access. In Case 1, endovascular intervention resulted in complete clinical resolution in the short term, demonstrating the effectiveness of this approach.
In conclusion, the cases described show that direct CCFs can occur spontaneously in elderly patients, even in the absence of trauma, and require high clinical suspicion. Early recognition of Dandy’s triad and sudden-onset orbital signs, combined with advanced imaging, is essential for rapid diagnosis and prompt referral for endovascular treatment. This approach is crucial for reducing morbidity, preserving visual acuity, and preventing potentially serious neurological complications.
REFERENCES
1. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous fistulas. J Neurosurg. 1985;62(2):248-56.
2. Ellis JA, Goldstein H, Connolly ES Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32(5):E9.
3. Halbach VV, Hieshima GB, Higashida RT, Reicher M. Carotid cavernous fistula: indications for urgent treatment. AJR Am J Neuroradiol. 1987;149(3):587-93.
4. Dandy WE. Orbital aneurysm of the internal carotid artery. Arch Surg. 1933;26(5):849-56.
5. Cloft HJ, Kallmes DF. Endovascular management of carotid cavernous fistulas. Neurosurg Clin N Am. 2005;16(3):447-55.
6. Gemmete JJ, Ansari SA, Gandhi D. Endovascular techniques for treatment of carotid-cavernous fistula. Neuroimaging Clin N Am. 2009;19(2):249-67.
7. Kupersmith MJ, Berenstein A, Choi IS, Nelson PK. Clinical features of spontaneous carotid cavernous fistulas. Arch Neurol. 1988;45(8):1066-71.
8. Miller NR. Differential diagnosis of orbital congestion. Trans Am Ophthalmol Soc. 1982;80:560-631.
9. Henderson AD, Miller NR. Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye (Lond). 2018;32(2):164-72.
| AUTHORS INFORMATIONS |
|
 |
»Isabella Passarelli Giabardo Marques https://orcid.org/0009-0004-1235-9800 http://lattes.cnpq.br/4382052210194962 |
 |
»Caio Henrique Peres Oliani https://orcid.org/0009-0003-3800-2984 http://lattes.cnpq.br/8416687727938491 |
 |
» Guilherme de Oliveira Aurich |
 |
» Guilherme Lopes Coelho https://orcid.org/0009-0009-9105-7064 http://lattes.cnpq.br/5954668772485257 |
 |
» Marcello Novoa Colombo Barboza |
 |
» Priscilla Fernandes Nogueira |
Funding: The authors declare no funding.
Ethics committee approval: Instituto do Câncer Brasil – ICBR (CAAE: 76124923.3.0000.0175).
Conflicts of interest: The authors declare no conflicts of interest.
Received on:
August 12, 2025.
Accepted on:
November 10, 2025.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket