

Breno de Mello Vitor
DOI: 10.17545/eOftalmo/2024.0028
Este artigo pertence à Edição Especial Abordagem Clínica da Baixa Visão: Estratégias de Reabilitação nas Principais Afe
ABSTRACT
This article reviews visual rehabilitation in keratoconus, a progressive corneal ectasia that typically affects young people and can cause significant functional limitations. Based on a review of recent literature, we describe the main types of contact lenses used in these patients, including soft toric lenses, rigid gas-permeable corneal lenses, piggyback systems, hybrid lenses, and scleral lenses, highlighting their indications, advantages, limitations, and potential complications. Next, we present the optical and biomechanical principles of intrastromal rings, the criteria for their selection, implantation techniques, visual outcomes, and associated adverse events. Finally, practical strategies for refraction in glasses and for contact lens wearers are discussed, with a focus on subjective visual quality and effective doctor-patient communication. The aim is to provide a concise, clinically applicable guide to optimize the visual rehabilitation of people with keratoconus.
Keywords: Keratoconus; Visual rehabilitation; Contact lenses; Intrastromal rings; Corneal cross-linking; Refraction.
RESUMO
Este artigo revisa a reabilitação visual no ceratocone, ectasia corneana progressiva que acomete, em geral, indivíduos jovens e pode causar importante limitação funcional. A partir de uma revisão da literatura recente, descrevem-se as principais modalidades de lentes de contato utilizadas nesses pacientes, incluindo lentes gelatinosas tóricas, rígidas gás-permeáveis corneanas, sistemas piggyback, lentes híbridas e esclerais, destacando indicações, vantagens, limitações e complicações. Em seguida, são apresentados os fundamentos ópticos e biomecânicos dos anéis intraestromais, seus critérios de seleção, técnicas de implantação, resultados visuais e possíveis eventos adversos. Por fim, discutem-se estratégias práticas de refração em óculos e sobre refração em usuários de lentes de contato, com foco na qualidade visual subjetiva e dedica-se atenção à efetiva comunicação médico–paciente. O objetivo é oferecer um guia conciso e aplicável à prática clínica para otimizar a reabilitação visual de pessoas com ceratocone.
Palavras-chave: Ceratocone; Reabilitação visual; Lentes de contato; Anéis intraestromais; Crosslinking corneano; Refração.
INTRODUCTION
Keratoconus is a progressive, non-inflammatory corneal ectasia characterized by stromal thinning and corneal protrusion, resulting in irregular astigmatism and increased higher-order optical aberrations, particularly coma. The disease typically begins in the second decade of life and follows a heterogeneous course. Clinically, it manifests as reduced visual acuity, image distortion, halos, and a significant impact on quality of life, most commonly affecting young people of school age or working age1,2.
For many years, the prevalence of keratoconus was estimated at approximately 1:2,000 inhabitants, based on limited diagnostic methods such as biomicroscopy and keratometry. More recent studies using Scheimpflug tomography and other high-resolution imaging techniques have shown that keratoconus is considerably more common, with prevalence rates ranging from 0.1% to over 3%–4% in different populations, depending on the diagnostic criteria employed3,4.
In a recent study using Scheimpflug tomography, Shabani et al. analyzed different definitions of keratoconus within the same cohort and demonstrated that prevalence varied from 0.19% to 9.29%, depending solely on the criteria used, highlighting the impact of diagnostic standardization4.
Recent reviews reinforce that keratoconus is the most common corneal ectasia, with an estimated prevalence of 120–265 per 100,000 inhabitants in the general population, and even higher in certain ethnic groups and specific regions, such as the Middle East and North Africa3. This higher frequency, combined with its early onset and potential for rapid progression in adolescents and young adults, makes keratoconus a significant public health concern. The disease is bilateral and asymmetrical in approximately 96% of cases5.
Modern management of keratoconus is based on three pillars:
1. Early diagnosis and risk stratification using corneal topography/tomography;
2. Control of progression, primarily with corneal collagen cross-linking;
3. Visual rehabilitation, using glasses, various types of contact lenses, intrastromal rings, and, in selected cases, corneal transplantation1,2,5.
This article focuses on visual rehabilitation in keratoconus, emphasizing: (a) contact lenses; (b) intrastromal rings; and (c) practical refractive strategies for these patients, integrating recent evidence from the medical literature1,2,5,6.
THE ROLE OF CONTACT LENSES IN VISUAL REHABILITATION
Contact lenses versus glasses
In the early stages of keratoconus, many patients can still achieve satisfactory visual acuity with spectacle correction or soft toric lenses, especially when astigmatism is relatively mild. As the ectasia progresses, with increasing corneal irregularity and higher-order aberrations, spectacle correction becomes insufficient, and patients often experience monocular diplopia, “ghosting,” and reduced contrast sensitivity. Advances in contactology over the past 5 years have emphasized the use of specialized scleral and corneal lenses4,7.
At these stages, contact lenses become the primary tool for visual rehabilitation. Recent reviews emphasize that contact lenses should be considered whenever vision cannot be corrected satisfactorily with glasses, and they are now the optical treatment of choice for most patients with moderate to advanced keratoconus4,8.
The decision to switch from glasses to contact lenses and the choice of lens type depend on several factors:
• Stage of the disease (assessed by topography, tomography, and pachymetry);
• Visual quality with glasses (functional or occupational limitations);
• Presence of central corneal scars;
• Previous tolerance to contact lenses;
• Ocular surface conditions (dry eye, allergy, blepharitis);
• Professional requirements and lifestyle1,2.
Fitting must be individualized, with a decision-making process that considers the morphology of the cone (nipple, oval, globular), location of the ectasia, minimum corneal thickness, and expected lens use1.
Types of contact lenses for keratoconus
Soft toric lenses and special designs
Soft toric lenses may be an option in early keratoconus, when corneal irregularity is still mild4. However, their ability to neutralize higher-order aberrations is limited, and visual quality is usually inferior to that achieved with rigid lenses4,9.
Soft lenses specifically “customized” for keratoconus, featuring increased central thickness and tailored designs, have been described, but they are primarily indicated for mild cases or for patients intolerant of rigid lenses who are willing to compromise between comfort and optical performance4.
The main features of soft toric lenses include:
• Advantages: greater initial comfort and rapid adaptation;
• Limitations: visual variability due to rotation of the toric axis, limited correction of corneal irregularity, and risk of hypoxia in thick lenses if Dk/t is inadequate4,9.
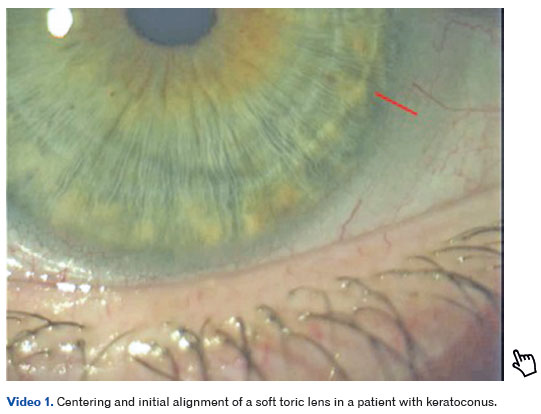
Video 1 demonstrates the positioning and centration of a soft toric lens after a few seconds of accommodation, highlighting corneal alignment and axis stability—key factors for achieving good visual quality in patients with keratoconus.
Rigid gas-permeable (RGP) corneal lenses
Corneal RGP lenses have been the gold standard for visual rehabilitation in keratoconus for decades2,4. They create a regular optical surface, with the tear film between the back of the lens and the cornea compensating for much of the irregularity. Studies show that RGP lenses provide better corrected visual acuity than glasses, with a significant reduction in coma and other higher-order aberrations4,9.
The current range of designs includes aspheric lenses, multicurve lenses, reverse-geometry lenses, and specific designs tailored to different cone morphologies. The choice of lens is guided by corneal topography and/or tomography, which inform the curvature, diameter, and base design, allowing adaptation for light apical contact or slight apical clearance, depending on the selected fitting philosophy1,5,9.
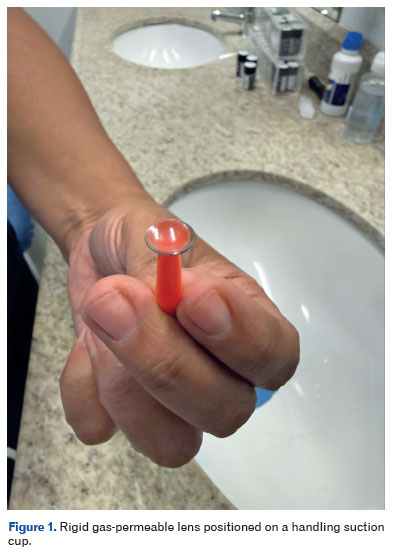
The main disadvantages include initial discomfort, the risk of apical microtrauma with excessive contact, and lens instability in very prominent or central cones. For better understanding, Figure 1 shows the anatomy of a rigid gas-permeable lens positioned on a suction cup used for insertion or removal, illustrating its shape, thickness, and transparency.
Piggyback systems
In cases where the patient achieves good visual acuity with an RGP lens but experiences intolerance due to discomfort or apical epithelial abrasions, a piggyback system—a high-Dk soft lens worn beneath the RGP lens—can be a useful strategy4,9. The soft lens protects the apex of the cone and improves comfort; however, it increases handling complexity and requires high-Dk materials in both lenses to minimize the risk of hypoxia4.
Hybrid lenses
Hybrid lenses feature a rigid gas-permeable central zone surrounded by a soft peripheral skirt, combining the optical performance of RGP lenses with the comfort of soft lenses. In keratoconus, specific designs allow proper lens centration over the cone, providing both stability and comfort4.
The main limitations include higher cost, the need for specialized care, and potential issues at the rigid–soft junction, such as tears or deposit formation. Despite these drawbacks, hybrid lenses remain a valuable option for patients who cannot tolerate pure corneal RGP lenses and are unable or unwilling to adapt to scleral lenses7.
Scleral and mini-scleral lenses
Scleral and mini-scleral lenses have gained prominence in recent years as highly effective tools for managing moderate to advanced keratoconus1,2,10. These lenses rest on the sclera and cover the entire cornea, creating a fluid reservoir between the lens and the epithelium that effectively neutralizes corneal irregularity10-14.
Studies have shown substantial and sustained improvements in visual acuity and quality of life with scleral lenses in keratoconus, even in advanced cases and post-keratoplasty corneas10,12,13,15.
The main advantages of scleral lenses include:
• Excellent optical quality due to the neutralization of aberrations;
• High comfort, as the lens rests on the conjunctiva/sclera;
• Positional stability, with minimal sensitivity to blinking.
Care during fitting involves controlling the central vault to achieve a balance that avoids both corneal contact and excessive fluid accumulation. Additionally, scleral alignment must be carefully assessed to prevent conjunctival or vessel blanching, while prioritizing high-Dk materials to reduce the risk of hypoxia10,11. These advances have elevated scleral lenses as a non-surgical mainstay in the management of keratoconus16.
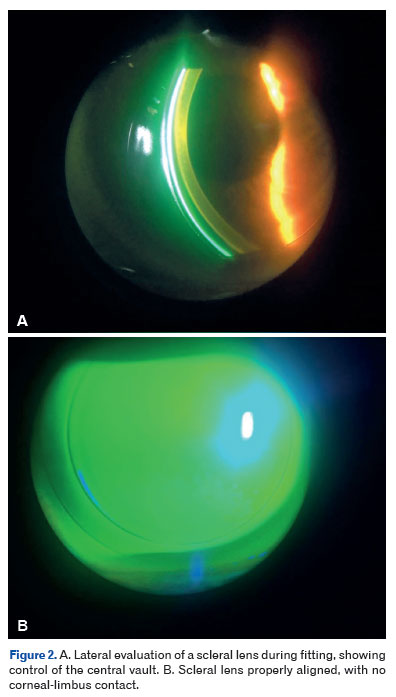
Figure 2A shows a lateral view of a scleral lens during the fitting process, highlighting the attention required to avoid excessive central clearance. Figure 2B shows the lens properly aligned, with no corneal-limbus contact, emphasizing the importance of careful assessment for achieving a safe and physiological fit.
It is important to note that, whenever possible, corneal RGP lenses should be tried before fitting a scleral lens, taking into account the dynamics of the lacrimal pump6.
PRACTICAL LENS FITTING STRATEGIES FOR KERATOCONUS
Contact lens fitting in keratoconus should be guided by three main elements: (a) tomographic and topographic data; (b) detailed biomicroscopic examination; and (c) subjective perception of vision and comfort.1,2,5
Choice of lens type according to cone morphology
Recent contact lens management guidelines provide practical algorithms for lens selection5,7,9:
• Small apical cone (nipple): Smaller-diameter corneal RGP lenses, with designs specific for keratoconus, are usually sufficient.
• Oval or paracentral cone: Larger-diameter RGP lenses, intralimbal lenses, or mini-scleral lenses tend to provide better centration and stability.
• Globus cone or extensive/post-surgical ectasia: Scleral lenses are generally the best option, as they can vault over large areas of corneal irregularity.
• Significant central scarring: Rigid lenses often improve vision substantially. If visual gain is limited by the opacity, keratoplasty may be considered1.
Oxygenation, duration of use, and complications
Chronic hypoxia is a major concern with contact lenses, particularly with thick soft lenses and scleral lenses with excessive vault. The use of high Dk/t materials is recommended, along with limiting wear time in low-oxygen environments and monitoring for signs of stromal edema, epithelial microcysts, and neovascularization10,11.
Common complications include apical abrasions with poorly fitting RGP lenses, sterile infiltrates, lens deposits, keratitis, and intolerance to maintenance solutions. Management strategies involve redesigning or refitting the lens, adjusting cleaning solutions, and addressing ocular surface comorbidities such as blepharitis, allergies, and dry eye5,7.
INTRACORNEAL RINGS IN KERATOCONUS
Optical and biomechanical principles
Intracorneal ring segments (ICRS) are PMMA implants placed in the mid-peripheral corneal stroma to reduce surface irregularities and decrease central corneal curvature. The implant increases the cornea’s peripheral circumference, promoting central flattening, reducing maximum keratometry values, and decreasing irregular astigmatism17,18.
The magnitude of the effect depends on several factors: the thickness, arc length (in degrees), and position of the segments, as well as the number of segments implanted, which may be one or two and can be positioned symmetrically or asymmetrically17,18.
Indications and case selection
The main indications for ICRS in keratoconus are17,18:
• Mild to moderate keratoconus with a clear cornea and adequate minimum stromal thickness at the implantation site (usually >400–450 µm, depending on the nomogram and device);
• Contact lens intolerance or poor visual quality with well-fitting lenses;
• Significant corneal irregularity that hinders or prevents proper contact lens fitting;
• Patient desire to reduce dependence on optical correction in selected cases.
Contraindications include dense central corneal scars, extreme stromal thinning, very advanced ectasia, severe ocular surface disease, and, in some cases, low endothelial cell counts17,18.
Updated nomograms incorporate factors such as cone location, degree of asymmetry, sphero-cylindrical refraction, pachymetry, and higher-order aberrations to determine the optimal number, thickness, and position of segments17,19.
Implantation techniques
Stromal tunnels for intracorneal ring segments can be created using either a mechanical technique or a femtosecond laser-assisted approach. Comparative studies suggest that the femtosecond laser provides greater accuracy in depth and diameter, reduces the risk of perforation, and allows more predictable centration, making it the preferred method in many centers14.
Recently, corneal allogenic intrastromal ring segments (CAIRS) have been proposed. These use donor corneal tissue instead of PMMA to reduce glare and complications associated with synthetic materials. Advantages of CAIRS include improved biocompatibility, lower extrusion rates, reduced risk of neovascularization, and minimal induction of stromal haze. Initial results are promising, although long-term studies are still lacking18.
Visual and topographic results
Narrative and systematic reviews show that ICRS provide14,16:
• An average improvement of 1–3 lines of corrected visual acuity;
• Reduction of maximum keratometry by 2–7 diopters, depending on the segment type and stage of ectasia20;
• Significant reduction in comatic and other higher-order aberrations.
Morales et al. note that ICRS are a minimally invasive option that can improve vision and potentially postpone or avoid keratoplasty in selected cases18. Recent studies in Brazil using asymmetric Keraring implants report consistent visual gains, significant reduction in astigmatism, and a low rate of serious complications19.
The combination of ICRS and corneal collagen cross-linking (CXL) is common practice. Evidence suggests that this combination can stabilize the ectasia and maintain the optical effects of the rings long-term, provided appropriate patient selection and surgical sequencing are followed17,18.
Complications
The main complications associated with ICRS include17,18:
Segment migration or extrusion;
Intraoperative anterior chamber perforation;
Deposits on the interface, night halos, and glare;
Epithelial defects over the segment;
Infectious keratitis.
Recent reviews indicate that the rate of serious complications is low when procedures are performed by experienced surgeons and properly planned17,18. In this context, ICRS have become an important tool in optical rehabilitation, particularly as a bridge between purely optical correction with contact lenses and keratoplasty.
REFRACTIVE TIPS FOR KERATOCONUS PATIENTS
Optical specificities
In keratoconus, higher-order aberrations, particularly vertical coma, have a significant impact on visual quality, even when measured visual acuity remains relatively good1,2,5. This implies that some patient complaints cannot be fully addressed with conventional sphero-cylindrical correction alone. Understanding this limitation is essential for managing patient expectations and accurately interpreting refractive outcomes.
Refraction in glasses
Although optimal visual rehabilitation in keratoconus often requires contact lenses, spectacle prescription remains relevant:
• As primary correction in the early stages of the disease;
• For specific tasks, such as reading or computer work;
• As a backup option in case of contact lens loss or intolerance.
Retinoscopy and objective refraction
Retinoscopy typically reveals the characteristic scissoring reflex of keratoconus, providing guidance for both the axis and approximate magnitude of astigmatism5. Autorefractors generally have low accuracy in these patients and should be used cautiously, primarily as an initial reference rather than a definitive measurement.
Subjective refraction - practical tips5,8,9
• Reduce the pupil diameter during the examination. Use a bright room with moderate table lighting to minimize the contribution of the most irregular corneal areas; dynamic refraction can also be employed.
• First determine the best spherical focus while controlling accommodation (fogging technique), then refine the cylinder.
• Avoid excessively high cylinder powers; for values above 4–5 D, it is often preferable to accept a slight loss of acuity in favor of greater comfort and tolerance.
• When possible, use a trial frame, as it more accurately reproduces actual conditions of use than a phoropter.
Consider anisometropia and aniseikonia. Very large interocular differences may require specific compensations or consideration of monocular predominance for certain tasks.
Utilize auxiliary formulas (such as empirical sphere–cylinder equivalence formulas) and allow the patient to actively participate in choosing the best cylindrical axis, adjusting it to achieve maximum visual sharpness.
Refraction in contact lens wearers
Over-refraction is a critical component of visual rehabilitation with contact lenses. Contemporary guidelines emphasize that careful over-refraction is decisive for achieving optimal visual outcomes, particularly with rigid and scleral lenses8,9.
General principles
• Perform over-refraction only after the lens has stabilized on the eye. For scleral lenses, it is recommended to wait approximately 60 min after insertion.
• For corneal RGP lenses, first address centering and lens movement issues before refining the refraction.
• For scleral lenses, evaluate the central clearance using a slit lamp; excessive vault can induce residual myopia11,12.
Practical technique
1. Begin with spherical refraction, identifying the best focus.
2. Assess the need for residual cylinder. If correction is required and clinically relevant, it can be addressed by:
• A front-surface toric lens;
• Spectacles over the contact lens, depending on the patient’s needs.
More advanced solutions, such as scleral lenses with customized optics guided by aberrometry, have been studied and may offer additional benefits in reducing higher-order aberrations, although they are not yet widely available19.
Strategies according to disease stage
Initial keratoconus
• Update refraction frequently, particularly in adolescents.
• Glasses or high-Dk soft toric lenses may be sufficient.
• Monitor disease progression with topography/tomography and consider early CXL if progression is detected1,2.
Moderate keratoconus
• Prioritize corneal RGP lenses designed for keratoconus, hybrid lenses, or scleral lenses, depending on cone morphology and the patient’s profile7,9.
• Provide spare glasses as a backup, even if visual acuity is lower than with contact lenses.
Advanced keratoconus
• RGP and scleral lenses are generally the main optical options10,12.
• If vision remains suboptimal with a well-fitted lens, or if contact lens use is contraindicated, consider ICRS to partially reshape the cornea. In extreme cases, assess the need for penetrating or deep anterior lamellar keratoplasty5,13.
Communication and patient expectations
Visual rehabilitation in keratoconus is an ongoing process. It is essential to explain to the patient that:
• Different strategies may be required throughout life (e.g., changing contact lens type, possible ICRS, CXL, or corneal transplant in specific cases).
• Even with optimized correction, vision may not be as “perfect” as in an eye without ectasia, particularly in low-light conditions.
• Controlling risk factors, especially avoiding eye rubbing and managing ocular allergies, is a crucial part of treatment and the preservation of vision1,6.
FINAL CONSIDERATIONS
Keratoconus is a relatively common corneal ectasia with early onset and significant functional impact. Recent epidemiological studies, including Brazilian cohorts, have reported higher prevalence rates than previously estimated, reinforcing the need for early diagnosis and systematic follow-up3,5.
In this context, visual rehabilitation plays a central role. Contact lenses, particularly corneal RGP and scleral lenses, are the primary tools for restoring visual function in most patients, providing consistent improvements in both visual acuity and quality of life7,10,12,13.
Intrastromal ring segments have been established as a valuable adjunctive surgical option to reduce corneal irregularity and, in many cases, delay the need for corneal transplantation17,19.
Finally, refraction in keratoconus, whether with spectacles or contact lenses, requires a refined approach, taking into account the limitations imposed by higher-order aberrations and emphasizing subjective visual quality. Recent literature highlights that the combination of modern optical techniques, adjuvant surgical interventions, and effective doctor-patient communication is fundamental to successful visual rehabilitation in this population1,2,6.
REFERENCES
1. Mannis M, Izquierdo L, HENRIQUEZ MA. (eds.). Keratoconus: diagnosis and management. Amsterdam: Elsevier, 2022.
2. Almodin E. (ed.). Keratoconus: a comprehensive guide to diagnosis and treatment. Cham: Springer, 2021.
3. Shabani H, van Dooren BTH, Meester-Smoor MA, Geerards AAJM, Klaver CCW, Ramdas WD. Different keratoconus definitions can lead to substantial prevalence disparities in population-based studies. Sci Rep. 2025;3483(15).
4. Moschos MM, Nitoda E, Georgoudis P, Balidis M,Karageorgiadis E, Kozeis N. Contact lenses for keratoconus – current practice. Open Ophthalmol J. 2017 Jul 31:11:241-251.
5. Barnett M, Mannis MJ. Contact lenses in the management of keratoconus. Cornea. 2011;30(12):1510-6.
6. Lipener, C. et al. Lentes de contato. São Paulo: Conexão Editora, 2023.
7. Almodin E. Ceratocone: um guia completo para diagnóstico e tratamento. Paraná: E.G. Almodin Educacional, 2025.
8. Contact lens update. Current perspectives in the management of keratoconus with contact lenses. 2023. Disponível em: https://contactlensupdate.com. Acesso em: 9 dez. 2025.
9. Keratoconus: diagnosis and management with spectacles and contact lenses. ResearchGate, 2022.
10. Lo H-L, Yeh S-I, Cheng H-C. Scleral contact lenses for visual rehabilitation in keratoconus and irregular astigmatism after refractive surgery. Taiwan J Ophthalmol. 2014;4:73-76.
11. Ozek D, Kemer OE, Altiaylik P. Visual performance of scleral lenses and their impact on ocular surface. Arq Bras Oftalmol. 2018;81(6):475-480.
12. Severinsky B, Behrman S, Frucht-Pery J, Solomon A. Scleral contact lenses for visual rehabilitation after penetrating keratoplasty. Cont Lens Anterior Eye. 2014;37(3):196-202.
13. Hadimani SR, Kaur H, Shinde AJ, Chottopadhyay T. Quality of life and vision assessment with scleral lenses in keratoconus. Saudi J Ophthalmol. 2023;38(2):173-178.
14. Ortenberg I, Behrman S. The role of scleral lens in ectatic corneas. Int J Kerat Ect Cor Dis. 2013;2(1):28-30.
15. Barone V, Petrini D, Nunziata S, Surio PL, Scarani C, Offi F, et al. Impact of scleral lenses on visual acuity and ocular aberrations in corneal ectasia: a comprehensive review. J Pers Med. 2024; 14(10):1051.
16. Mushtaq A, Alvi I. Long-term effectiveness of scleral lens treatment in the management of keratoconus: a systematic review. Cureus. 2025;17(1):e77102.
17. Hayat UK, Shiwani HA, Memon D, Walkden A. Intracorneal ring segments in keratoconus: a narrative literature review. Clin Ophthalmol. 2025 Jul 11:19:2249-2257.
18. Morales P, Durán JA. Advances in intracorneal ring segment (ICRS) implantation for keratoconus: a comprehensive literature review, clinical insights, and future prospects. J Clin Med. 2025;14(13):4454.
19. Amaral DC, Alves MR, Guedes J, Feitosa Filho HN, Aguiar EHC, Correa DC, et al. Asymmetric intracorneal ring segments for the management of keratoconus:a systematic review and meta-analysis. J Curr Ophthalmol. 2025;36(4):325-341.
20. Silva FBD, Daher ND.Influência da espessura dos segmentos de anel corneano na correção do astigmatismo ceratométrico em pacientes com ceratocone. Rev Bras Oftqalmol. 2021 ;80(6):e0053.
| AUTHOR INFORMATION |
|
 |
»Breno de Mello Vitor https://orcid.org/0009-0003-3430-1135 http://lattes.cnpq.br/0826752576668237 |
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
November 21, 2025.
Accepted on:
December 10, 2025.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket