

Antomir Santos Pereira; José Gabriel Abreu Moreira; Raul de Carvalho Cavalcante Filho; Vinícius Rothier Duarte Neves; Danilo Ramos Stropp; Haroldo de Lucena Bezerra
DOI: 10.17545/eOftalmo/2024.0022
ABSTRACT
PURPOSES: This meta-analysis aimed to systematically evaluate the diagnostic accuracy and clinical performance of artificial intelligence applied to smartphone-captured images for screening diabetic retinopathy.
METHODS: The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy (PRISMA-DTA) guidelines and was registered in the PROSPERO database (CDR420251011626). Searches were conducted in six databases (Scopus, Embase, Web of Science, MEDLINE, Cochrane Library, and LILACS). Studies using AI implemented in smartphone-based imaging were included. Methodological quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool, and publication bias was evaluated using Deeks' test. Statistical analysis was performed using a bivariate random-effects model to estimate sensitivity, specificity, positive and negative likelihood ratios, diagnostic odds ratio, and the area under the hierarchical receiver operating characteristic curve.
RESULTS: Ten studies were included, evaluating a total of 5,370 eyes. Sensitivity and specificity were 91.4% and 89.4%, respectively. Diagnostic accuracy was high (area under the curve: 0.956), and heterogeneity was low.
CONCLUSIONS: Artificial intelligence applied to smartphone-derived images appears promising for diabetic retinopathy screening, particularly in settings with limited access to ophthalmologists.
Keywords: Artificial intelligence; Diabetic retinopathy; Diagnostic test; Ophthalmoscopy; Smartphone.
RESUMO
OBJETIVOS: Esta meta-análise avaliou sistematicamente a precisão diagnóstica e o desempenho clínico da inteligência artificial aplicada a imagens capturadas por smartphones na triagem da retinopatia diabética.
MÉTODOS: A revisão seguiu as diretrizes Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Diagnostic Test Accuracy (PRISMA-DTA) e foi registrada no banco PROSPERO (CDR420251011626). A busca foi realizada em seis bases de dados (Scopus, Embase, Web of Science, MEDLINE, Cochrane Library e LILACS). Foram incluídos estudos que utilizaram inteligência artificial acoplada a smartphones. A qualidade metodológica foi avaliada com a ferramenta Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) e o viés de publicação foi investigado pelo teste de Deeks. A análise estatística utilizou um modelo bivariado de efeitos aleatórios para estimar sensibilidade, especificidade, razão de verossimilhança positiva e negativa, razão de chances diagnósticas e área sob a curva da característica de operação do receptor hierárquico.
RESULTADOS: Dez estudos foram incluídos, totalizando 5.370 olhos avaliados. A sensibilidade foi de 91,4% e a especificidade de 89,4%, com alta acurácia diagnóstica (área sob a curva de 0,956) e baixa heterogeneidade.
CONCLUSÕES: Conclui-se que o uso de inteligência artificial em imagens de smartphones é promissor na triagem da retinopatia diabética, especialmente em contextos com acesso limitado a oftalmologistas.
Palavras-chave: Inteligência artificial; Retinopatia diabética; Teste diagnóstico; Oftalmoscopia; Smartphone.
INTRODUCTION
Diabetes mellitus (DM) is a group of metabolic diseases characterized by hyperglycemia1. Currently, around 537 million people are living with diabetes, and this number is expected to surpass 750 million by 2045, with 23 million of them in Brazil alone2. Hyperglycemia has damaging effects on the eyes3, making diabetic retinopathy (DR) the most common complication of DM and one of the leading causes of avoidable blindness in the productive adult population4. DR is a microangiopathy involving microvascular obstruction or leakage and occurs in patients with chronic, uncontrolled blood glucose. After two decades of disease, it is found in more than 95% of patients with type 1 DM and in more than 60% of those with type 2 DM5.
In recent years, advances have been made both in the development of medical tools and in awareness of the importance of DR screening, especially in developed countries6. In these countries, dilated fundus examination, considered the gold standard for DR screening, plays a fundamental role in early detection of the disease. It helps prevent serious complications, including blindness, and contributes to significant reductions in healthcare costs for patients with DM7,8. However, its accuracy is considerably lower when performed by non-specialist physicians8.
In this context, the use of artificial intelligence (AI) has emerged as a lower-cost alternative, as it enables automated analysis of large volumes of retinal images and reduces dependence on specialists for initial screening. One important application of this technology is the use of smartphone-attached cameras, which offer a portable and affordable solution that expands access to early DR detection in resource-limited settings9.
Although several studies have explored the effectiveness of AI and portable devices for DR screening, results remain variable. A systematic review with meta-analysis of six studies evaluated AI-based DR screening using smartphones in 3,931 eyes, with most studies conducted in India (five) and one in Brazil10. Although that review contributed to understanding AI’s role in this context, it had limitations, including limited geographical diversity and a small number of AI programs evaluated.
More recently, with the growing popularity of AI, there has been a significant increase in studies assessing AI for disease screening, especially for DR, reflecting the expanding use of this technology in diverse scenarios. Compared to the aforementioned systematic review with meta-analysis10, the present review offers a broader scope, including 5,370 eyes and a more diverse set of studies from five countries: Armenia (one study), Brazil (two), Dominica (one), Mexico (one), and India (five). This greater heterogeneity makes the evaluation more representative of AI performance across different populations and health systems, supporting broader generalization of the results. Furthermore, to date, no meta-analyses on this topic have been published in Portuguese, reinforcing the need for an updated review to fill this gap.
Therefore, the aim of this meta-analysis was to systematically evaluate the diagnostic accuracy and clinical performance of AI-based tools for DR screening. The analysis of these findings will contribute to a better understanding of AI’s role in DR screening and may support the implementation of effective strategies in clinical practice, particularly in resource-limited settings.
METHODS
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy (PRISMA-DTA) guidelines11. The study protocol was previously published and is registered with PROSPERO (CDR420251011626).
Search strategy
A comprehensive search was performed in several databases, including Scopus, Embase, Web of Science, MEDLINE, Cochrane Library, and LILACS, up to January 28, 2025. Boolean operators were applied appropriately to link the different keywords, and Medical Subject Headings (MeSH) were extensively incorporated to ensure search breadth.
The search strategy was: (“diabetes” OR “diabetes complications” OR “diabetic retinopathy” OR “diabetic” OR “diabetic complication”) AND (“artificial intelligence” OR “neural network” OR “predictive algorithm” OR “deep learning” OR “deep neural network” OR “DNN” OR “machine learning” OR “deep Bayesian” OR “bimodal learning” OR “contrast learning” OR “pyramid learning” OR “convolutional neural network” OR “CNN”) AND (“smartphone” OR “smartphone-based” OR “mobile-based” OR “handheld” OR “iPhone” OR “mobile camera” OR “mobile”).
Selection criteria
The selection criteria followed the PICOT framework: 1. Patients with type 1 or type 2 diabetes mellitus, of any age and from any location. 2. Use of smartphones coupled with optical adapters and AI algorithms for DR screening. 3. Ophthalmoscopy performed by specialists. 4. Primary diagnostic parameters: True Positive (TP), False Positive (FP), False Negative (FN), and True Negative (TN). 5. Diagnostic accuracy studies, diagnostic clinical trials, and observational implementation studies published in Portuguese or English, with no time restriction.
Studies were excluded if they met any of the following criteria: 1. Systematic reviews and meta-analyses. 2. Case reports or case series. 3. Editorials or letters to the editor. 4. Conference abstracts. 5. Lack of a valid reference standard. 6. Absence of quantitative diagnostic accuracy data.
Study selection was performed independently by two authors using the Rayyan platform to minimize selection bias12. When eligibility could not be determined based on the title and abstract alone, full texts were reviewed. Any disagreements were resolved with the involvement of a third, more experienced author.
Data extraction
Data extraction was conducted independently by two authors, and any disagreements were resolved by consensus. Data were collected using Microsoft Excel.
Extracted information included key methodological and clinical characteristics of the studies: study name (author and year), study country, study design, total sample size (n), number of unclassifiable individuals, gender distribution (female/male), mean participant age (in years), use of mydriasis, number of photographic fields per eye, AI program used, reference standard applied, and diagnostic parameters (TP, FP, FN, and TN).
Methodological quality
The methodological quality of the included studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool13, which evaluates risk of bias and applicability across four domains: flow and timing, reference standard, index test, and patient selection.
Risk-of-bias assessment was conducted independently by two authors, with differences resolved by consensus.
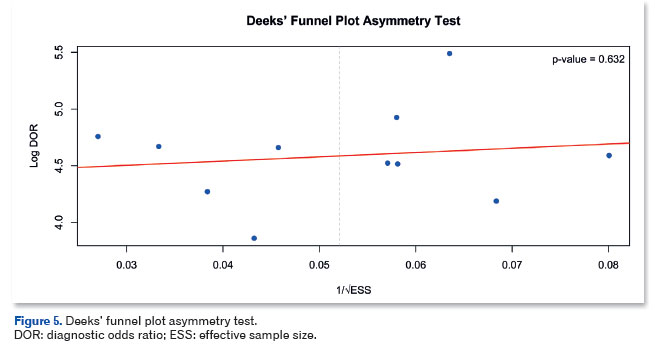
Publication bias was evaluated using Deeks’ funnel plot asymmetry test, which is specific for bivariate meta-analyses of diagnostic accuracy. A p-value <0.1 was considered indicative of publication bias.
Statistical analysis
Statistical analyses were performed using RStudio software (version 4.4.2). A bivariate random-effects meta-analysis model was used to jointly assess sensitivity and specificity. Heterogeneity was evaluated using an adapted I2 statistic for bivariate models, as proposed by Zhou and Dendukuri14. Fixed effects (sensitivity and specificity), their correlation, the positive likelihood ratio (LR+), and the negative likelihood ratio (LR−) were also calculated.
A hierarchical summary receiver operating characteristic (HSROC) curve was generated to summarize diagnostic performance, and the area under the curve (AUC) was used to assess overall model accuracy.
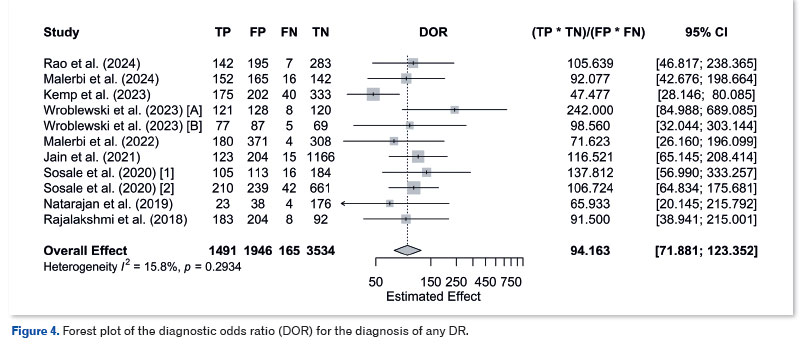
The diagnostic odds ratio (DOR) was calculated and presented in a forest plot, with heterogeneity assessed using I2 and the Q-test.
A significance level of 5% was applied to all statistical analyses.
RESULTS
Study selection
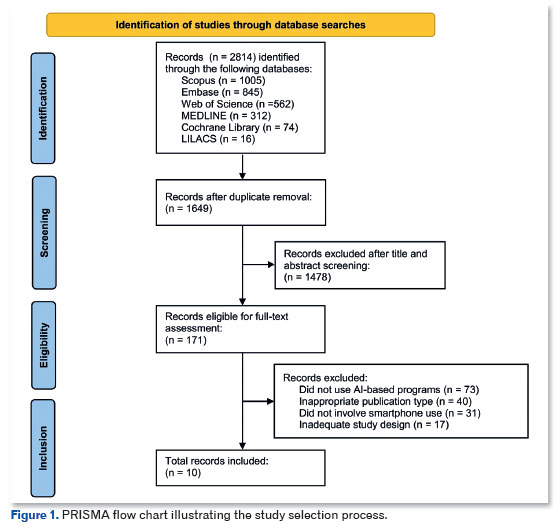
A systematic search was conducted in six databases (Scopus, Embase, Web of Science, MEDLINE, Cochrane Library, and LILACS), which initially identified 2,814 potentially relevant records. After removing 1,165 duplicate articles, 1,649 unique records remained. Of these, 1,478 were excluded during title and abstract screening. The full texts of the remaining 171 articles were assessed, and 161 were excluded because they did not meet the inclusion criteria. Ultimately, 10 studies were included in the final meta-analysis9,15-23. The study selection process is illustrated in Figure 1, following the PRISMA flowchart format.
Characteristics of the studies
As shown in Table 1, a total of 10 eligible studies published between 2018 and 2024 were included, representing 5,370 eyes, with sample sizes ranging from 231 to 1,378 participants. The number of unclassifiable images varied across the studies, with minimum values of 0 and maximum values of 145. One study was analyzed using two different approaches and is referred to as Wroblewski 2023 [A] and Wroblewski 2023 [B] throughout the analyses.
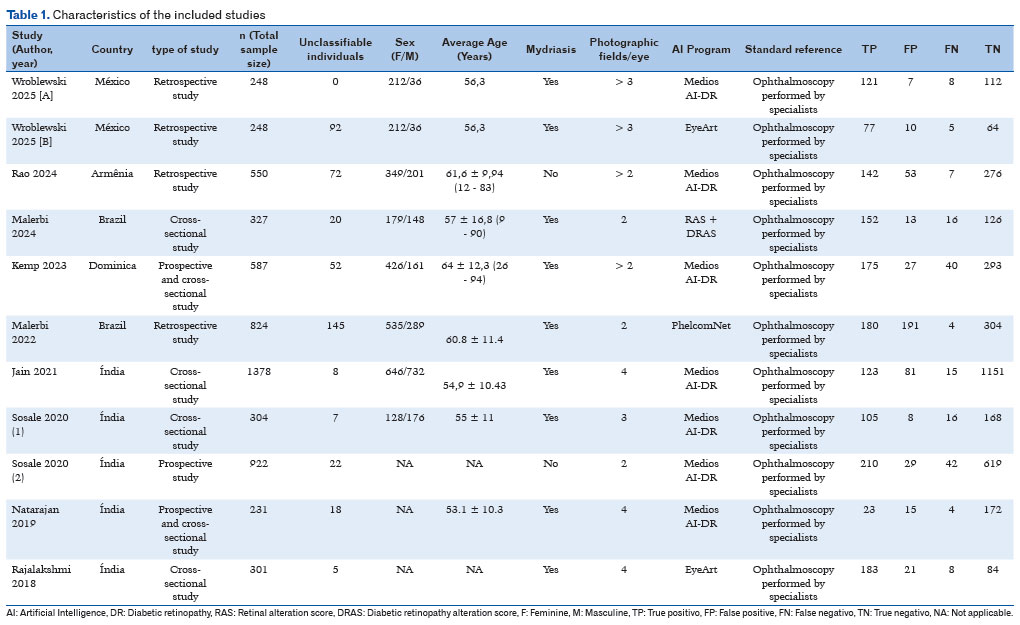
The studies were conducted in several countries, including Armenia, Brazil, Dominica, Mexico, and India. Regarding study design, five were cross-sectional, four were retrospective, and three were prospective, with two employing a mixed approach that combined prospective and cross-sectional designs9,22.
The use of mydriasis for image acquisition varied, being applied in eight studies9,15,17-20,22,23. The number of photographic fields per eye ranged from two to more than four, with all studies capturing at least two fields.
The AI programs evaluated included a variety of algorithms and software systems such as Medios AI-DR, EyeArt, PhelcomNet, and RAS + DRAS. In all studies, the reference evaluation was conducted by a human grader.
Quality assessment
The methodological quality of the included studies was assessed using the QUADAS-2 tool13, and the results are presented in Figure 2. Among the 10 included studies9,15-23, two showed unclear risk in the flow and timing domain15,20,and three were considered to have unclear risk in the patient selection domain20,22,23.
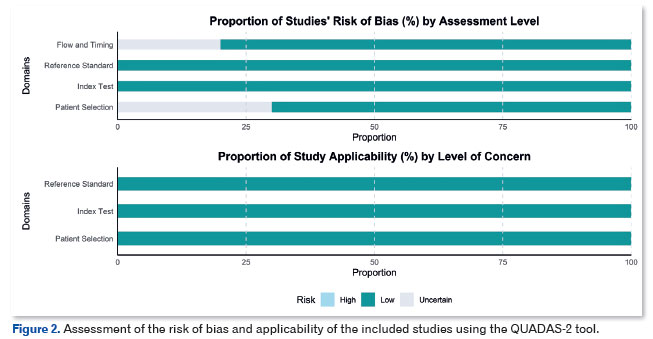
Regarding applicability, although some concerns were noted, particularly in the areas of patient selection and flow and timing, the overall quality of the studies was considered acceptable for clinical interpretation of the findings.
Results of effectiveness
A bivariate random-effects meta-analysis was performed (Figure 3). The fixed-effect coefficients indicated a mean sensitivity of 0.914 (95% CI: 0.871–0.944) and a mean specificity of 0.894 (95% CI: 0.840–0.931). The estimated LR+ was 8.64 (95% CI: 5.59–13.36) and the LR− was 0.10 (95% CI: 0.06–0.15).
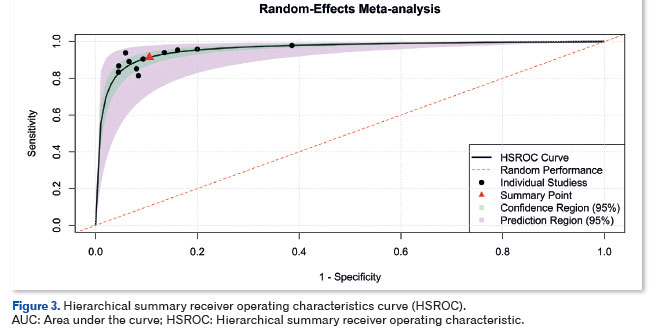
Variability among the studies was represented by a standard deviation of 0.705 for sensitivity and 0.758 for specificity. The correlation between these metrics was high (0.946), indicating a strong dependence between them.
The AUC was 0.956, demonstrating high overall diagnostic performance of the models. Heterogeneity assessed via I2 was 18.3%, indicating low heterogeneity.
The diagnostic odds ratio (DOR) estimated by the random-effects model was 94.16 (95% CI: 71.88–123.35), indicating high discriminative capacity of the diagnostic tests. Heterogeneity was low, with I2 = 1 5.8% and a Q-test p-value of 0.2934, suggesting no substantial variability among the included studies (Figure 4).
Publication bias
The Deeks’ funnel plot asymmetry test (Figure 5) did not show evidence of significant publication bias (p = 0.632), suggesting that the absence of negative or lower-impact studies does not compromise the validity of the meta-analysis findings.
DISCUSSION
The aim of this systematic review and meta-analysis was to evaluate the effectiveness of AI programs applied to images captured by smartphones for DR screening. By compiling and critically analyzing relevant studies, this review sought to provide insights that may assist healthcare professionals in making informed decisions about incorporating these technologies into clinical practice.
The results demonstrated high diagnostic accuracy, with a sensitivity of 0.914 (95% CI: 0.871–0.944) and specificity of 0.894 (95% CI: 0.840–0.931). The LR+ was 8.64 (95% CI: 5.59–13.36) and the LR– was 0.10 (95% CI: 0.06–0.15), indicating strong ability to confirm and exclude disease. Variability among the studies was moderate (SD ≈ 0.7 for both metrics), and the correlation between sensitivity and specificity was high (0.946). The AUC of 0.956 and the DOR of 94.16 (95% CI: 71.88–123.35) further demonstrated excellent discriminative performance. When compared to the IDx-DR device, the first US Food and Drug Administration (FDA)-approved medical device using AI to detect DR in adults with diabetes, which achieved a sensitivity of 0.874 and a specificity of 0.89524, the slightly higher sensitivity observed in the present analysis suggests that smartphone-based AI programs may be a valuable alternative for large-scale screening.
Comparing these findings with a previous meta-analysis21, which reported sensitivity and specificity of 0.88 and 0.915 respectively for detecting any DR, reveals similar values, with slightly higher sensitivity in the present study. This may suggest better ability to confirm disease. Additionally, the LR+ in the present study (12.2) was higher, indicating stronger rule-in capability, while the LR− values were nearly identical (0.11), showing comparable effectiveness in excluding DR. The DOR of the previous analysis was 111.7, that is, higher than that of the present meta-analysis (94.16), suggesting that the previous models had slightly better diagnostic discrimination. However, the differences were not substantial, and both studies point to a high performance of AI algorithms in screening for DR.
The assessment of the risk of bias using QUADAS-2 showed that most studies presented low risk in the “Reference Standard” and “Index Test” domains, indicating methodological robustness in these aspects. However, the “Patient Selection” domain showed a significant proportion of studies with high or unclear risk of bias, which may limit the external validity of the results. With regard to applicability, the elevated level of concern in some studies suggests that the findings should be interpreted with caution in specific clinical contexts. It is recommended that future research prioritize study designs that minimize these biases to ensure greater sample representativeness.
The incorporation of AI into DR screening could have a significant impact on optimizing workflows in settings that lack technological resources and specialized staff, enabling more efficient diagnosis and referral to secondary care by ophthalmologists. Because DR affects approximately one in three people with diabetes25, its early detection is essential to prevent severe complications such as blindness. However, diagnosing the disease can be challenging, as it may be confused with neurological disorders or other ophthalmic pathologies26.
Thus, the clinical application of AI in DR screening has emerged as a fundamental tool for reducing diagnostic errors and increasing accuracy in initial assessments. Although the automated and accessible assessment provided by AI using smartphone images was not directly compared with methods such as retinography or optical coherence tomography in this meta-analysis, it appears to be a promising strategy for optimizing DR screening, especially in resource-limited settings27,28.
The use of this new screening method, particularly its incorporation into primary care, which serves the majority of patients with diabetes in Brazil, could result in effective implementation and a favorable cost-benefit for the country by facilitating diagnostic access. However, future studies are needed to evaluate cost-effectiveness in greater depth and to guide health policies28.
Despite promising advances, further research must be conducted in larger centers to evaluate AI and its clinical application in DR, thereby ensuring its safe and effective implementation. Finally, the findings reinforce the potential of AI as a support tool to assist physicians in DR screening, enabling appropriate referral with the aim of reducing the burden on specialized services and improving outcomes for individuals with diabetes.
In conclusion, this systematic review with meta-analysis provides important insights into the applicability of AI using images captured by smartphone devices for diabetic retinopathy screening. The performance of AI in DR screening was shown to be excellent, with high sensitivity and specificity. The potential of AI to help detect diabetic retinopathy (though not to determine its severity) was demonstrated, particularly in settings where specialized care is limited.
In addition, the incorporation of this technology can optimize workflows in primary care and allow more efficient referral for specialist assessment. Therefore, the results presented herein are promising; however, future research involving trials in larger centers with a higher number of participants and greater population heterogeneity is necessary to confirm these findings and support broader and safer clinical implementation.
REFERENCES
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010 Jan;33 Suppl 1(Suppl 1):S62-9. Erratum in: Diabetes Care. 2010 Apr;33(4):e57.
2. International Diabetes Federation. IDF Diabetes Atlas 9th Edition [Internet]. diabetesatlas.org. 2021. Available from: https://diabetesatlas.org/data/en/
3. Lutty GA. Effects of diabetes on the eye. Invest Ophthalmol Vis Sci. 2013;54(14):ORSF81-7.
4. Teo ZL, Tham YC, Yu M, Chee ML, Rim TH, Cheung N,et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology. 2021;128(11):1580-91.
5. Bortoli JQ, Silber PC, Picetti E, Silva CF da, Pakter HM. Retinografia como forma de rastreio de retinopatia diabética em hospital terciário do Sistema Único de Saúde. Rev Bras Oftalmol. 2022;81:e0057.
6. Padhy SK, Takkar B, Chawla R, Kumar A. Artificial intelligence in diabetic retinopathy: A natural step to the future. Indian J Ophthalmol. 2019;67(7):1004-1009.
7. Malerbi F, Andrade R, Morales P, Travassos S, Rodacki M, Bertoluci M. Manejo da retinopatia diabética. Diretriz Oficial da Sociedade Brasileira de Diabetes (2023). DOI: 10.29327/557753.2022-17, ISBN: 978-85-5722-906-8.
8. O’Hare JP, Hopper A, Madhaven C, Charny M, Purewell TS, Harney B, et al. Adding retinal photography to screening for diabetic retinopathy: a prospective study in primary care. BMJ. 1996;312(7032):679-82.
9. Kemp O, Bascaran C, Cartwright E, McQuillan L, Matthew N, Shillingford-Ricketts et al. Real-world evaluation of smartphone-based artificial intelligence to screen for diabetic retinopathy in Dominica: a clinical validation study. BMJ Open Ophthalmol. 2023;8(1):e001491.
10. Hasan SU, Siddiqui MAR. Diagnostic accuracy of smartphone-based artificial intelligence systems for detecting diabetic retinopathy: A systematic review and meta-analysis. Diabetes Res Clin Pract. 2023;205:110943.
11. McInnes MDF, Moher D, Thombs BD, McGrath TA, Bossuyt PM; and the PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA. 2018;319(4):388-396. Erratum in: JAMA. 2019;322(20):2026..
12. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
13. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et, al; QUADAS-2 Group. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-36.
14. Zhou Y, Dendukuri N. Statistics for quantifying heterogeneity in univariate and bivariate meta-analyses of binary data: the case of meta-analyses of diagnostic accuracy. Stat Med. 2014;33(16):2701-17.
15. Wroblewski JJ, Sanchez-Buenfil E, Inciarte M, Berdia J, Blake L, Wroblewski S, et al. Diabetic Retinopathy Screening Using Smartphone-Based Fundus Photography and Deep-Learning Artificial Intelligence in the Yucatan Peninsula: A Field Study. J Diabetes Sci Technol. 2025;19(2):370-376.
16. Rao DP, Savoy FM, Sivaraman A, Dutt S, Shahsuvaryan M, Jrbashyan N, et al. Evaluation of an AI algorithm trained on an ethnically diverse dataset to screen a previously unseen population for diabetic retinopathy. Indian J Ophthalmol. 2024;72(8):1162-7.
17. Malerbi FK, Nakayama LF, Melo GB, Stuchi JA, Lencione D, Prado PV, et al. Automated Identification of Different Severity Levels of Diabetic Retinopathy Using a Handheld Fundus Camera and Single-Image Protocol. Ophthalmol Sci. 2024;4(4):100481.
18. Malerbi FK, Andrade RE, Morales PH, Stuchi JA, Lencione D, de Paulo JV, et al. Diabetic Retinopathy Screening Using Artificial Intelligence and Handheld Smartphone-Based Retinal Camera. J Diabetes Sci Technol. 2022;16(3):716-23.
19. Jain A, Krishnan R, Rogye A, Natarajan S. Use of offline artificial intelligence in a smartphone-based fundus camera for community screening of diabetic retinopathy. Indian J Ophthalmol. 2021;69(11):3150-4.
20. Sosale B, Sosale AR, Murthy H, Sengupta S, Naveenam M. Medios- An offline, smartphone-based artificial intelligence algorithm for the diagnosis of diabetic retinopathy. Indian J Ophthalmol. 2020;68(2):391-395.
21. Sosale B, Aravind SR, Murthy H, Narayana S, Sharma U, Gowda SGV, et al. Mobile-based Artificial Intelligence Algorithm in the detection of Diabetic Retinopathy (SMART) study. BMJ Open Diabetes Res Care. 2020;8(1):e000892.
22. Natarajan S, Jain A, Krishnan R, Rogye A, Sivaprasad S. Diagnostic Accuracy of Community-Based Diabetic Retinopathy Screening With an Offline Artificial Intelligence System on a Smartphone. JAMA Ophthalmol. 2019;137(10):1182-1188.
23. Rajalakshmi R, Subashini R, Anjana RM, Mohan V. Automated diabetic retinopathy detection in smartphone-based fundus photography using artificial intelligence. Eye (Lond). 2018 Jun;32(6):1138-1144.
24. Office of the Commissioner. FDA permits marketing of artificial intelligence-based device to detect certain diabetes-related eye problems [Internet]. U.S. Food and Drug Administration. 2018. Available from: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-artificial-intelligence-based-device-detect-certain-diabetes-related-eye
25. Ministério da Saúde (BR). Portaria Conjunta nº 17, de 1º de outubro de 2021. Aprova o Protocolo Clínico e Diretrizes Terapêuticas da Retinopatia Diabética [Internet]. Brasília (DF): Ministério da Saúde; 2021. Acessar em https://bvsms.saude.gov.br/bvs/saudelegis/saes/2021/poc0017_16_12_2021.html
26. Ahmed J, Ward TP, Bursell SE, Aiello LM, Cavallerano JD, Vigersky RA. The sensitivity and specificity of nonmydriatic digital stereoscopic retinal imaging in detecting diabetic retinopathy. Diabetes Care. 2006;29(10):2205-9.
27. Carneiro LFSA, Carvalho PS, Santos PHE, Delfino DGS, Mourão MS, Gonçalves AS, et al. Rastreamento da retinopatia diabética pelo médico generalista na Atenção Primária de Saúde do Brasil. Rev Bras Oftalmol. 2024;83:e0014.
28. Oliveira LES de, Silva MC da, Santiago RVC de, Benevides CA, Cunha CCH, Matos AG. Diagnóstico da retinopatia diabética por inteligência artificial por meio de smartphone. Rev Bras Oftalmol. 2024;83:e0006.
| AUTHORS INFORMATIONS |
|
 |
» Antomir Santos Pereira https://orcid.org/0009-0009-2488-4158 http://lattes.cnpq.br/0237563895156365 |
 |
» José Gabriel Abreu Moreira https://orcid.org/0009-0005-1645-1820 http://lattes.cnpq.br/7424259581681244 |
 |
» Raul de Carvalho Cavalcante Filho https://orcid.org/0009-0001-9795-7700 http://lattes.cnpq.br/4843763196727858 |
 |
» Vinícius Rothier Duarte Neves https://orcid.org/0009-0004-4230-013X http://lattes.cnpq.br/9057096884239460 |
 |
» Danilo Ramos Stropp https://orcid.org/0009-0003-6415-5722 https://lattes.cnpq.br/5495492066379401 |
 |
» Haroldo de Lucena Bezerra https://orcid.org/0000-0002-2946-1244 http://lattes.cnpq.br/8824480892150126 |
Funding: The authors declare no funding.
Conflicts of interest: The authors declare no conflicts of interest.
Received on:
January 10, 2023.
Accepted on:
November 12, 2025.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket