

Amanda Prado; Graciela Scalco Brum; Eduardo de Almeida Rosales
DOI: 10.17545/eOftalmo/2024.0008
ABSTRACT
Graves' orbitopathy is an organ-specific autoimmune reaction in which antibodies react against orbital cells, resulting in inflammation of various structures, including the extraocular muscles. Diplopia and strabismus are the limiting consequences of this condition. This study included a case of a 55-year-old female patient with restrictive strabismus and diplopia after orbital decompression due to Graves' orbitopathy. The symptoms were affecting her daily activities. The clinical outcomes were extremely satisfactory. Furthermore, a potential improvement in the patient's quality of life can be achieved by considering the chronology of interventions and using adequate surgical techniques.
Keywords: Graves' orbitopathy; Esotropia; Strabismus; Diplopia; Ocular surgery.
RESUMO
A orbitopatia de Graves decorre de uma reação autoimune órgão-específica, na qual anticorpos reagem contra células orbitais, resultando inflamação de várias estruturas, incluindo os músculos extraoculares. Diplopia e estrabismo são consequências limitantes desse processo. O presente artigo relata o caso de uma paciente feminina de 55 anos com estrabismo restritivo e diplopia, afetando seu dia a dia, após descompressão orbitária por Orbitopatia de Graves, cujo desfecho clínico-cirúrgico foi extremamente satisfatório. O respeito à cronologia das intervenções e adequada técnica cirúrgica oferecem potencial melhora na qualidade de vida do paciente através de ganho funcional e estético, reforçado pelo presente relato.
Palavras-chave: Orbitopatia de Graves; Esotropia; Estrabismo; Diplopia; Cirurgia ocular.
INTRODUCTION
Graves' disease is an autoimmune disease characterized by the production of autoantibodies against the thyroid-stimulating hormone receptor (TSH-R) resulting in thyroid dysfunction. Most patients with Graves' orbitopathy (GO) usually present with an endocrinological condition called hyperthyroidism in addition to periocular condition. Hyperthyroidism is an excess of hormones produced by the gland. However, GO may also be present in euthyroid or hypothyroid patients1. This association suggests the presence of a common antigen between the thyroid gland and orbital tissues.
The presence of TSH receptors in orbital fibroblasts justifies the clinical presentation1. Upper eyelid retraction is the most common sign of the disease, which occurs in up to 90% of all patients resulting from hyperactivity of the Mullerian muscle. This muscle has sympathetic innervation and is responsible for eye opening. Proptosis occurs in up to 60% of all cases. GO is the main cause of bilateral and unilateral proptosis in this population. Rarely, an increase in adipose and muscular tissue in the orbit can result in the compression of the optic nerve and optic neuropathy1,2.
GO often involves the extraocular muscles in the form of restrictive strabismus due to muscle enlargement secondary to fat infiltration between the muscle fibers. The most affected muscles are as follows (in descending order): (1) inferior rectus, (2) medial rectus, (3) superior rectus, and (4) lateral rectus1,2. Strabismus may cause anomalous head positions and diplopia in 26%-45% of patients. Moreover, these symptoms may significantly impair the performance of daily activities3-5. As is emphasized by the literature and this report, the consideration of the chronology of interventions and the use of adequate surgical techniques can potentially improve the patient's quality of life through functional and esthetic gains.
CASE REPORT
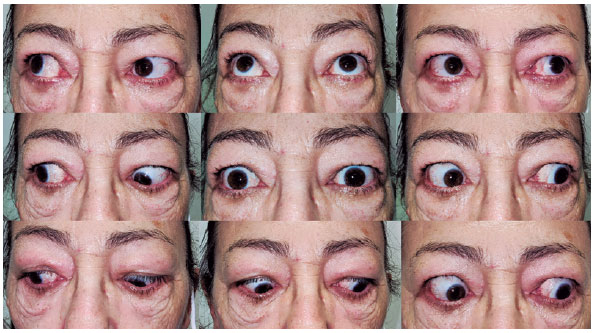
This study included a female patient aged 55 years old who is a smoker in abstinence for 6 months and was diagnosed with GO 7 years ago. The patient presented with strabismus and diplopia after orbital decompression was performed (Figure 1). During the preliminary examination, she presented with esotropia (ET) of 35–40 prismatic diopters in the left eye, as measured using the Krimsky method. She also reported diplopia in the primary position of gaze (PPG) (i.e., levo- and supraversions). These findings were supported by muscle restriction and are consistent with the literature as the medial and inferior rectus muscles are most frequently involved.

During surgery, a bilateral 6-mm recoil of the medial rectus muscles was performed. At 1 month after surgery, during follow-up evaluation, the patient expressed significant esthetic and functional satisfaction. Diplopia was not observed during examination based on the PPG. She had a small residual deviation of ET OE of 8 SD and hypotropia of 4 SD in the prismatic cover test (Figure 2).
DISCUSSION
Despite the surgical challenges represented by strabismus in GO, the patient was satisfied with the esthetic results and resolution of diplopia in the PPG and the most cardinal positions of gaze. The surgery could rehabilitate the patient to return to her daily activities3-5.
It is important to recognize the existence of two phases in GO. The first phase is denominated the “dynamic phase”, followed by the “static phase”. The dynamic phase focuses on regulating inflammation and stabilizing the condition. In mild cases, nonsteroidal anti-inflammatory drugs are initiated. The therapeutic arsenal in moderate to severe cases comprised oral corticosteroids, pulse therapy, and radiotherapy. Recent studies investigated new monoclonal antibodies in the dynamic phase. In the static phase, it is possible to correct proptosis, strabismus, and upper eyelid restriction1,2.
Achieving the desired therapeutic outcome requires the consideration of the correct sequence of procedures. Strabismus correction should only be performed after orbital decompression as indicated. If the patient wishes, correction of upper eyelid retraction can be performed after strabismus surgery. In this final stage, it is possible to choose between surgical treatment and botulinum toxin.
Stability of the underlying clinical disease and abstaining from preoperative smoking are also essential for success. Tobacco is associated with GO decompensation and is directly linked to a worse prognosis and higher incidence of strabismus. Furthermore, smoking increases the risk of developing GO by up to seven times in addition to being related to more severe presentations of the disease1,2,6,7.
REFERENCES
1. Website. 2020–2021 BCSC Basic and Clinical Science CourseTM. Disponível em: https://www.aao.org/education/bcscsnippetdetail.aspx?id=035a3b5b-1b6f-4d1e-bf76-98898b4b46b7. Acesso em: 31/1/2024.
2. Bowling B. Kanski Oftalmologia Clínica: Uma abordagem sistêmica. Editora GEN Guanabara Koogan. 2017.
3. Jellema HM, Braaksma-Besselimk Y, Limpens J, von Arx G, Wiersinga WM, Mourits MP. Proposal of success criteria for strabismus surgery in patients with Graves' orbitopathy based on a systematic literature review. Acta Ophthalmol. 2015;93(7):601-6.
4. Jellema HM, Merckel-Timmer E, Kloos R, Saeed P, Mourits MP. Quality of life improves after strabismus surgery in patients with Graves' orbitopathy. Eur J Endocrinol. 2014;170(5):785-9.
5. Leite CA. Efeito da correção cirúrgica da exoftalmia na motilidade ocular extrínseca de pacientes com orbitopatia de Graves: comparação entre a descompressão orbitária inferomedial e a descompressão orb. (Universidade de São Paulo, 2020). doi:10.11606/T.5.2020.tde-21072021-162457.
6. Rajendram R, Bunce C, Adams GGW, Dayan CM, Rose GE. Smoking and strabismus surgery in patients with thyroid eye disease. Ophthalmology. 2011;118(12):2493-7.
7. Nunery WR, Martin RT, Heinz GW, Gavin TJ. The association of cigarette smoking with clinical subtypes of ophthalmic Graves' disease. Ophthalmic Plast Reconstr Surg. 1993;9(2):77-82.
AUTHORS INFORMATIONS |
|
 |
» Amanda Prado http://orcid.org/0000-0002-2622-4876 lattes.cnpq.br/5810497598236197 |
 |
» Graciela Scalco Brum http://orcid.org/0009-0007-1961-5987 lattes.cnpq.br/6172173241473556 |
 |
» Eduardo de Almeida Rosales http://orcid.org/0009-0005-4174-8546 lattes.cnpq.br/7567539753502961 |
Funding: No specific financial support was available for this study.
Project number and institution responsible for the opinion of the Research Ethics Committee: CAAE 77562524.2.0000.5335 | Hospital Santa Casa de Porto Alegre, Porto Alegre, RS, Brasil.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
April 9, 2024.
Accepted on:
April 15, 2024.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket