

Ana Beatriz Ferreira do Amaral Antunes1; Henrique Dall Agnol Gonçalves2; Luiz Fernando Interaminense Garbers1
DOI: 10.17545/eOftalmo/2023.0034
ABSTRACT
Iridocorneal endothelial syndrome includes a group of rare eye disorders divided into three clinical variations that are difficult to differentiate. This disease affects predominantly women (ratio of 5:1) in the 3rd and 5th decades of life and almost exclusively in Caucasian individuals. In this report we present a rare case of the clinical variant progressive (essential) iris atrophy of the iridocorneal endothelial syndrome in a 22-year-old male patient. He presented for a routine ophthalmological examination without visual complaints or previous history of eye disease. Gonioscopy showed the high peripheral anterior synechiae in the left eye, which were tent-like in several quadrants, and no changes in the right eye. There is no effective treatment that demonstrates regression of the disease; the aim is to prevent and treat its potential complications.
Keywords: Glaucoma; Corneal endothelium; Corneal disease; Iridocorneal endothelial syndrome; Case reports
RESUMO
A síndrome iridocorneana endotelial representa um grupo de distúrbios oculares raros, sendo dividida em três variações clínicas de difícil diferenciação. Essa doença tem prevalência no sexo feminino 5:1 na 3ª e 5ª década de vida e quase que exclusivamente em caucasianos. O presente estudo tem por objetivo relatar um raro caso da variante clínica atrofia progressiva (essencial) da íris da síndrome iridocorneana endotelial em um paciente masculino de 22 anos. Este apresentou-se para um exame de rotina oftalmológica sem queixas visuais ou história pregressa de doenças oftalmológicas. A gonioscopia do olho esquerdo apontou sinéquias anteriores periféricas altas, em tenda em diversos quadrantes, e em olho direito não apontou alterações. Não há um tratamento efetivo que demonstre regressão da doença, busca-se prevenir e tratar suas possíveis complicações.
Palavras-chave: Glaucoma; Endotélio corneano; Doença da córnea; Síndrome endotelial iridocorneana; Relatos de caso
Iridocorneal endothelial syndrome (ICE SD) consists of a group of rare eye disorders that have as a common denominator the proliferation of corneal endothelial cells that migrate to the iris and the iridocorneal angle. There are three clinical variations that are difficult to differentiate and the disease affects predominantly women (ratio of 5:1) in the 3rd and 5th decades of life, and almost exclusively in Caucasian individuals. It is frequently associated with glaucoma, either due to obstruction of the angle by cell proliferation or to contraction of the Descemet’s membrane over the iris, resulting in the formation of peripheral anterior synechiae1,2.
Corneal endothelial cells do not divide after birth, they remain in a state of quiescence G1 phase of mitosis due to the presence of cyclin-dependent kinase inhibitors. There is a triggering factor that causes the loss of control of these endothelial cells undergoing the cell cycle, leading to dysregulation in which endothelial cells proliferate and act as epithelial cells2. The clinical variant progressive (essential) iris atrophy is characterized by the thinning and atrophy of the iris stroma, resulting in defects throughout its thickness. The early formation of peripheral anterior synechiae can lead to pupillary distortions (corectopia) and angle closure, thereby increasing intraocular pressure (IOP) due to a pretrabecular block1,3. Finally, the progressive increase in tension in the iris stroma results in more atrophy of the iris and the formation of full-thickness holes that are characteristic of the disease2.
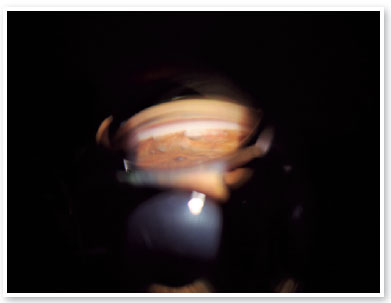
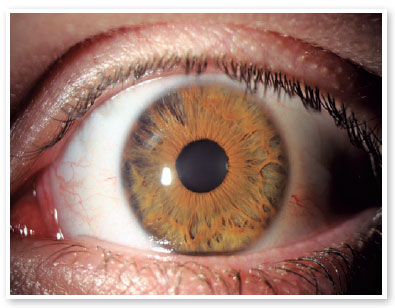
A 22-year-old male patient presented for a routine examination without visual complaints or previous history of ophthalmological diseases. Gonioscopy of the left eye (OS) showed high peripheral anterior synechiae (Figure 1), which were tent-like in several quadrants, and no changes in the right eye (OD). Optical coherence tomography (OCT) of the peripapillary nerve fiber layer, fundus photography, corneal specular microscopy, automated campimetry, and computerized keratoscopy were requested. The results were all normal. In view of the clinical presentation of progressive, unilateral closure in a young man with biomicroscopic features typical of ICE (Figure 2), the diagnosis of the ICE SD variant progressive (essential) iris atrophy was made. Specular microscopy, ultrasound biomicroscopy, OCT, pachymetry, and computerized visual field testing are useful to detect the aforementioned alterations1.
There is no effective treatment that demonstrates regression of the disease, the aim being to prevent and manage its potential complications. Drainage devices are used in most cases of uncontrolled IOP, but there is the option of trabeculectomy with mitomycin C. Cases of corneal edema are managed by tension control and, if necessary, by penetrating keratoplasty or endothelial keratoplasty, which yield good results and a rapid recovery of the patient4,5.
This was a case of essential iris atrophy, a clinical variant of ICE SD, in which the patient’s presentation diverged from the usual epidemiological pattern, namely because this was a young man. The patient was instructed to undergo routine ophthalmology follow-up.
REFERENCES
1. Estacia CT, Gameiro Filho AR, Faccenda PG, Negri RV, Chianello DT, Alves MAS. Síndrome Iridocorneana Endotelial: relato de caso da Variante Chandler. Rev Bras Oftalmol. 2017;76(4):207-9.
2. Silva L, Najafi A, Suwan Y, Teekhasaenee C, Ritch R. The iridocorneal endothelial syndrome. Surv. Ophthalmol. 2018; 63(5):665-76.
3. Pereira JAB, Camarota IC. Atrofia essencial da íris associada à hipertrofia congênita do epitélio pigmentar da retina. Rev Bras Oftalmol. 2011;70(3):185-7.
4. Silva DDB, Matos MAG, Pessoa SAR, Avila AC, Dantas H. Síndrome de Cogan-Reese: relato de um caso. Medicina (Ribeirão Preto). 2000;33(1):82-87.
5. Price MO, Price FW Jr. Descemet stripping with endothelial keratoplasty for treatment of iridocorneal endothelial syndrome. Cornea. 2007;26(4):493-7.
AUTHORS INFORMATIONS



Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
December 5, 2022.
Accepted on:
June 11, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket