

Juliana Prazeres1; Luiz Filipe Lucatto2
DOI: 10.17545/eOftalmo/2023.0003
Este artigo pertence à Edição Especial Dominando a arte da cirurgia vitreorretiniana: técnicas e dicas
Submacular hemorrhage (SMH) is a significant cause of irreversible visual loss, and there are various techniques available to manage it, including pneumatic displacement with or without intravitreal tissue plasminogen activator (tPA), pars plana vitrectomy with subretinal tPA and gas tamponade, and submacular surgery with vitrectomy and retinotomy for clot extraction1.
In cases of massive SMH, pars plana vitrectomy (PPV) and injection of tPA into the subretinal space is generally the preferred treatment. This can be done by injecting tPA directly into the subretinal space or by creating a macular retinal detachment to deliver tPA through the same retinotomy2,3.
We present a case of an 85-year-old male with a single eye and a decrease in vision in his right eye over the past 3 days. He had a past ocular history of AMD with a disciform scar and EPR tear after anti-VEGF injection 4 years ago in the left eye. He had an extensive submacular hemorrhage secondary to AMD with a visual acuity of count fingers.
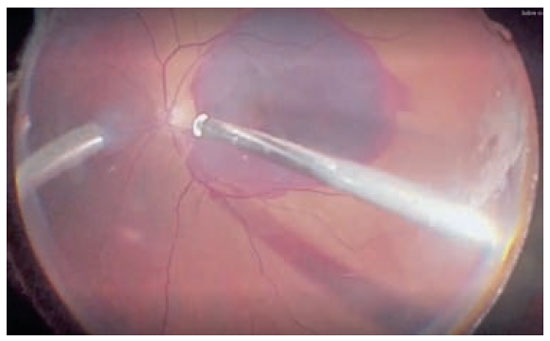
We decided to perform a PPV with subretinal tPA injection. After core vitrectomy and posterior hyaloid detachment, we first injected BSS into the subretinal space using a 38g cannula adapted in the viscous fluid control unit with a MicroDose injection kit (medOne).
Before injecting BSS into the subretinal space, it is important to reduce the intraocular pressure and reduce the pressure in the VFI system. It is important to check the flow before injection, as a low flow speed is sufficient to create a retinal detachment without the risks associated with a macular hole or damage to EPR.
After the subretinal BSS injection, we injected 0.2mL of tPA (25µm/0.1mL) solution into the subretinal space using the same retinotomy. A fluid-air exchange was performed, and the patient was instructed to lie down in a supine position for 20 minutes to increase the time for the tPA to act.
REFERENCES
1. Kishikova L, Saad AAA, Vaideanu-Collins D, Isac M, Hamada D, El-Haig WM. Comparison between different techniques for treatment of submacular haemorrhage due to Age-Related Macular Degeneration. Eur J Ophthalmol. 2021;31(5):2621-2624.
2. Wilkins CS, Mehta N, Wu CY, Barash A, Deobhakta AA, Rosen RB. Outcomes of pars plana vitrectomy with subretinal tissue plasminogen activator injection and pneumatic displacement of fovea-involving submacular haemorrhage. BMJ Open Ophthalmol. 2020 Mar 16;5(1):e000394.
3. Hirashima T, Moriya T, Bun T, Utsumi T, Hirose M, Oh H. Optical coherence tomography findings and surgical outcomes of tissue plasminogen activator-assisted vitrectomy for submacular hemorrhage secondary to age-related macular degeneration. Retina. 2015;35(10):1969-78.
AUTHOR’S INFORMATION
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
November 30, 2022.
Accepted on:
December 18, 2022.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 MP4
MP4
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket