

Flavio Fernandes Villela1; Daniela Lima de Jesus2; Fernando Eiji Sakassegawa Naves3; Fabrício Witzel de Medeiros4; Murilo Barreto Souza5; Gustavo Victor6; Milton Ruiz Alves7
DOI: 10.17545/e-oftalmo.cbo/2017.79
ABSTRACT
OBJECTIVE: To compare the efficacy of visual screening using the Snellen chart to that of refractive screening using the SpotTMVision Screener for detecting the causal factors for amblyopia in a pre-school-aged population (4–6-year-old children).
METHODS: In total, 97 pre-school-aged children enrolled in city and state day care centers underwent visual screening exams [uncorrected monocular visual acuity(VA) cut-off point of ≤0.7 and/or a difference in VA of two or more lines between the two eyes] and refractive screening exams (cut-off points: hypermetropia ≥ +3.00 D, myopia ≥ −0.75 D, and astigmatism ≥ −0.75 D). All children then underwent a complete ophthalmologic exam, and the refractive error was measured using cycloplegic manual retinoscopy.
RESULTS: Among the children with refractive errors above the adopted cut-off point, the estimated percentages of those who were not referred for a complete ophthalmologic exam were 46.4% in the case of the visual screening method and 17.9% in the case of the refractive screening method. The visual screening method using the Snellen chart exhibited a sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 58.6%, 64.7%, 41.5%, and 78.6%, respectively. The refractive screening method using the SpotTM Vision Screener exhibited a sensitivity, specificity, PPV, and NPV of 92.8%, 35.2%, 37.1%, and 92.3%, respectively.
CONCLUSION: Refractive screening using the SPOTTMVision Screener was more effective than visual screening using the Snellen chart for detecting the causal factors for amblyopia in the studied population.
Keywords: Visual Acuity; Diagnostic Techniques, Ophthalmological; Refraction, Ocular; Vision Screening; Child, Preschool
RESUMO
OBJETIVO: Comparar a eficácia do rastreamento visual com tabela optométrica de Snellen com o rastreamento refrativo com o SpotTM Vision Screener na detecção de fatores causadores de ambliopia em uma população de pré-escolares com 4-6 anos de idade.
MÉTODOS: Foram submetidas a rastreamento visual 97 crianças pré-escolares matriculadas em creches municipais e estaduais (ponto de corte: AV monocular sem correção ≤ 0,7 e/ou diferença duas linhas de Snellen entre os olhos) e rastreamento refrativo (ponto de corte: hipermetropia ≥ +3,00 D, miopia ≥ -0,75 D e astigmatismo ≥ -0,75 D). Todas as crianças foram submetidas a exame oftalmológico completo e mensuração do erro refrativo sob cicloplegia com retinoscopia manual em faixa.
RESULTADOS: Os percentuais estimados da não referência para exame oftalmológico completo das crianças com erros de refração acima do ponto de corte estabelecido foram: 46,4% para o rastreamento visual e 17,9% para o rastreamento refrativo. O método de rastreamento visual com tabela optométrica de Snellen apresentou valores de sensibilidade, especificidade, valor preditivo positivo (VPP) e valor preditivo negativo (VPN), respectivamente, 58,6%, 64,7%, 41,5% e 78,6%. O método de rastreamento refrativo com o SpotTM Vision Screener apresentou valores de sensibilidade, especificidade, VPP e VPN, respectivamente, 92,8%, 35,2%, 37,1% e 92,3%.
CONCLUSÃO: O rastreamento refrativo com o SPOTTM Vision Screener foi mais eficaz que o rastreamento visual com tabela optométrica de Snellen na detecção de fatores causados de ambliopia na população estudada.
Palavras-chave: Acuidade visual; Técnicas de Diagnóstico Oftalmológico; Refração Ocular; Seleção visual; Pré-escolar
INTRODUÇÃO
Amblyopia is characterized by a uni-or bilateral reduction in visual acuity (VA) resulting from an inadequate visual experience during the first year of life1,2. A multicenter study by the Pediatric Eye Disease Investigator Group demonstrated that among 3–6-year-old children, anisometropia and strabismus were each responsibles for approximately 40% of cases of amblyopia and jointly for 20%of cases3. The study demonstrated that in children, the average refractive error was +4.52 D in amblyopic eyes and +2.83 D in contralateral eyes; the average value in the contralateral eyes was high among strabismic children (+3.54 D) and low among anisometropic children3. Strabismus is the most relevant risk factor for amblyopia in the first year of life. Anisometropia alone or accompanied with strabismus is the most relevant factor for amblyopia from 3 years of age. In the fifth year of life, anisometropia is responsible for amblyopia in two-thirds of children1,3.
In 2003, the Vision Screening Committee of the American Association for Pediatric Ophthalmology and Strabismus established guidelines for issuing reports on the results of visual screening studies performed using automated equipment4. These new technologies have been developed to identify children with risk factors for amblyopia (strabismus, anisometropia, and/or high bilateral refractive error)5.
Brazil’s public healthcare system is not yet structured for ophthalmologic care for pre-school-aged children; human resources are limited in terms of professionals who can promote ocular health, and there is a lack of physical infrastructure and equipment for refractive exams6. The Brazilian Council of Ophthalmology (CBO) has stated the need for new measures to control the increasing demand and to broaden the access of children to ophthalmology services7. One way to increase ophthalmologic care among pre-school-aged children includes incorporating new technology into the screening processes. This study aimed to compare the efficacy of visual screening using the Snellen chart to that of refractive screening using the SpotTM Vision Screener for detecting the causal factors for amblyopia in a pre-school-aged population (4–6-year-old children) using the criteria adopted by the CBO for determining cut-off points in refractive and visual screening methods8,9.
METHODS
This prospective study was approved by the Brazilian National Research Ethics Committee. The study population comprised 97 pre-school-aged children (4–6 years old) enrolled in public schools or day care centers in São Paulo. They were examined at the Clinical Hospital of the School of Medicine of the University of São Paulo (HCFMUSP) from March to December 2014. The informed consent form was obtained from the parents or legal guardians of the children.
An ophthalmologic exam was performed in the following sequence: i) the training and measurement of uncorrected monocular VA in a well-lit area using the Snellen chart 5 m away from the child, with the lines 0.8 and 1.0 positioned at the eye level of the child; ii) obtaining three measurements using the SpotTM Vision Screener to measure refractive errors; iii) cycloplegic manual retinoscopy (one drop of 1% cyclopentolate, followed by an exam 30 min later); iv) biomicroscopy of the ocular surface and anterior segment using a slit lamp; and v) dilated fundus examination.
The SpotTM Vision Screener used in this study was supplied by LOKTAL Medical Electronics, São Paulo, Brazil (software version 1.1.51). The cut-off point for the uncorrected visual screening was as follows: uncorrected monocular VA≤ 0.7 and/or a difference in VA of two or more lines between the eyes. The cut-off point for refractive screening was as follows: hypermetropia ≥ +3.00 D; myopia ≥ −0.75 D, and/or astigmatism ≥ −0.75 D.
The demographic data and results of the exams were recorded in individual files, and database spreadsheets were created in Microsoft Excel®. The qualitative variables were presented in terms of absolute and relative values. The quantitative variables were presented in terms of their central tendency and dispersion. The screening methods were evaluated by comparing their sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The results and respective 95% confidence intervals were presented as percentages. The level of statistical significance was set at p<0.05.
RESULTS
The average age and standard deviation of the 97 pre-school-aged children (44 boys and 53 girls) was 58 ± 5 months. VA was not determined in four children (4.1%), two were strabismic, nine (9.23%) were diagnosed with possible amblyopia, and two (2.1%) were confirmed as having amblyopia.
Table 1shows the distribution of the pre-school-aged children into two groups according to the cut-off point adopted for visual screening.
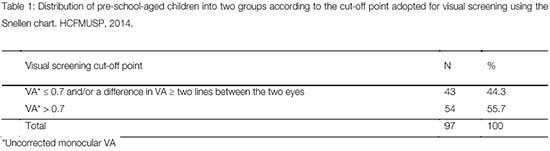
Table 2 shows the distribution of the pre-school-aged children into two groups according to the cut-off point adopted for refractive screening.
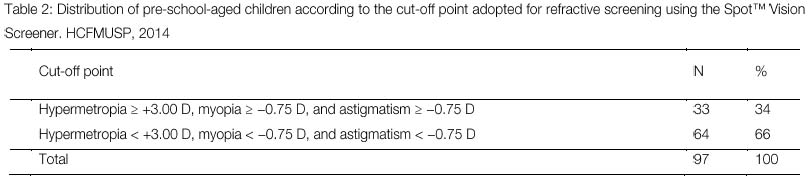
Table 3 shows the number of children diagnosed with a refractive error above the adopted cut-off point as well as the number and percentage of children not identified by the visual and refractive screening methods.

In total, 13 children (46.4%) were not identified by the visual screening method using the Snellen chart, and five (17.9%) were not identified by the refractive screening using the SpotTM Vision Screener.
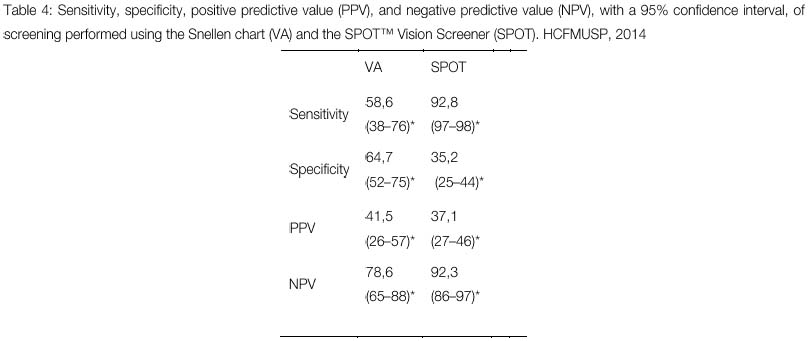
Table 4 shows the sensitivity, specificity, PPV, and NPV of the visual screening performed using the Snellen chart and of therefractive screening performed using the SpotTM Vision Screener.
DISCUSSION
In this study, using visual screening with the Snellen chart as part of a complete ophthalmologic exam, we found that 43 children (44.3%) exhibited uncorrected monocular VA≤ 0.7 and/or a difference in VA of two or more lines between the two eyes, whereas543 (55.7%) exhibited uncorrected monocular VA > 0.7 (Table 1). Using refractive screening with the SpotTM Vision Screener as part of a complete ophthalmologic exam, we found that 33 children (34.1%) exhibited hypermetropia ≥ +3.00 D, myopia ≥ −0.75 D, and/or astigmatism ≥ −0.75 D, whereas 64 (65.9%) exhibited hypermetropia<+3.00 D, myopia < −0.75. D, and/or astigmatism<−0.75 D (Table 2). Of the 28 children diagnosed with refractive errors above the cut-off point, 13 (46.4%) failed to be identified by visual screening and five (17.9%) failed to be identified by refractive screening (Table 3). Differences in the values obtained after using the two types of screening methods (visual and refractive) are directly correlated with the manner in which the information was obtained. Visual screening depends on subjective information and is subject to the children's verbal skills, neural and psychomotor development, understanding of the exam, reading skills and speed, and other factors, all of which influence the information obtained when measuring VA. Measurements obtained in the refractive screening method do not depend on the children’s understanding of the method or on subjective information obtained during the exam. This exam is performed with no physical contact with the child; however, it may be influenced by the changes in the transparency of ocular structures or by theenvironment, such as excessive lighting, which may alter the pupil size and hamper photorefraction10.
In the current study, two children (2.1%) were found to be strabismic. This result is consistent with those of manyprevious multicenter, prospective, and population-based studies that have confirmed an approximately 2% prevalence of amblyopia11,12,13. However, the prevalence of risk factors for amblyopia (15%–20%) found in this study was much higher than that previously reported14,15,16. These findings clarify that most children with risk factors for amblyopia do not develop amblyopia; this fact has been confirmed in other longitudinal observational studies on children with issues identified using visual screening17. Therefore, it is imperative that guidelines be updated so that ophthalmologists can detect risk factors that distinguish children who are going to develop amblyopia from those who are not5. Among children with anisometropia who are younger than 3 years, the prevalence of amblyopia appears to be correlated with the magnitude of anisometropia18. However, among children older than 3 years, the prevalence of amblyopia appears to be relatively constant, although the extent of amblyopia increases with age, and a high refractive error appears to be sufficient to increase the extent,but not the prevalence, of amblyopia19.
The current study found sensitivity values of 58.6% inthe case of visual screening using the Snellen chart and of 92.8% in the case of refractive screening using the SpotTM Vision Screener (Table 4). Highly sensitive tests are the most important at the beginning of the diagnostic process, such as that in clinical outreach programs, school screening programs, and exams offered outside of medical environments, when a large number of diagnostic possibilities are being considered and if the goal is to reduce the likelihood of failure in identifying all positive cases. Specificity values were 64.7% in the case of visual screening and 35.2% in the case of refractive screening. Specificity is defined as the percentage of pre-school-aged children who do not need to undergo a complete ophthalmologic exam (true negatives), as detected by the method, among all children detected as negatives by the gold standard method (complete ophthalmologic exam). PPVs were 41.5% in the case of visual screening and 37.1% in the case of screening using the SpotTM Vision Screener. PPV is the percentage of children detected as true positives among all children with a positive diagnosis, i.e., it expresses the probability of a given child with positive screening to present a refractive error above the adopted cut-off point. The test indicated that 37.1% of the children referred for the ophthalmologic exam with the SpotTM Vision Screener did, in fact, present a risk factor for amblyopia. It is important to note that modifications to the reference criteria would change sensitivity and PPV. NPVs were 78.6% in the case of visual screening and 92.3% in the case of refractive screening. NPV is the percentage of children detected as true negatives among all children with a negative diagnosis, i.e., it expresses the probability that a given child with negative screening will not present a refractive error above the adopted cut-off criteria.
The external validity of this study was hindered by the fact that the pre-school-aged children were examined at a hospital (HCFUSP) and not at their schools or day care centers. The cut-off points used for visual and refractive screening methods were those provided by the CBO, which hampered the comparison of the results of this study to those of other studies in the literature. However, under the current study conditions, the refractive screening method using the SPOTTM Vision Screener was the most effective in detecting the risk factors for amblyopia in the pre-school-aged population (4–6-years-old children).
REFERENCES
1. Birch EE. Amblyopia and binocular vision. Prog Retin Eye Res. 2013;33:67-84. http://dx.doi.org/10.1016/j.preteyeres.2012.11.001
2. Birch EE, Holmes JM. The clinical profile of amblyopia in children younger than 3 years age. J AAPOS. 2010;14:494-7. http://dx.doi.org/10.1016/j.jaapos.2010.10.004
3. Pediatric Eye Disease Investigator Group. The clinical profile of moderate amblyopia in children younger than 7 years. Arch Ophthalmol. 2002;120:281-7. http://dx.doi.org/10.1001/archopht.120.3.281
4. Donahue SP, Arnold RW, Ruben JB, AAPOS Vision Screening Committee. Preschool vision screening: what should we detecting and how should we report it? Uniform guidelines for reporting results of preschool vision screening studies. J AAPOS. 2003;7:314-6. http://dx.doi.org/10.1016/S1091853103001824
5. Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB. Guidelines for automated preschool vision screening: a 10-year, evidence, evidence-based update. J AAPOS. 2013;17:4-8. http://dx.doi.org/10.1016/j.jaapos.2012.09.012
6. Ferraz FHS, Hirai F, Schellini AS. Estimativas da magnitude e do custo da correção da baixa visão por erro de refração não corrigido no Brasil. In: Alves MR, Nishi M, Carvalho KM, Ventura LMV, Kara-José N, editores. Refração ocular: uma necessidade social. Rio de Janeiro: Cultura Médica; 2014. p. 35-47.
7. Carvalho KM, Minguini N, Alves MR. Detecção e tratamento dos erros de refração no grupo etário de 0 a 6 anos. In: Alves MR, Nishi M, Carvalho KM, Ventura LMV, Kara-José N, editores. Refração ocular: uma necessidade social. Rio de Janeiro: Cultura Médica; 2014. p. 55-66.
8. Alves MR, Kara-José N. Manual de orientação -veja bem Brasil. São Paulo: Conselho Brasileiro de Oftalmologia; 1998.
9. Alves MR, Kara-José N. Manual de instruções. Campanha Nacional de Prevenção de Cegueira e Reabilitação Visual. Salvador: Conselho Brasileiro de Oftalmologia; 1998.
10. SpotTM Vision Screener by Welch Allyn. [Internet]. [cited 2017 Mar 1]. Available from: https://www.welchallyn.com/en/products/categories/physical-exam/eye-exam/vision-screeners/spot-vision-screener.html
11. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115:1229-36. http://dx.doi.org/10.1016/j.ophtha.2007.08.001
12. Friedman DS, Repka MX, Katz J, Giordano L, Ibironke J, Hawse P, Tielsch JM. Prevalence of amblyopia and strabismus in white and african american children aged 6 through 71 months the Baltimore Pediatric Eye Disease Study. Ophthalmology. 2009;116:2128-34. http://dx.doi.org/10.1016/j.ophtha.2009.04.034
13. Pai AS, Rose KA, Leone JF, Sharbini S, BurlutskyG, Varma R, Wong TY, Mitchell P. Amblyopia prevalence and risk factors in australian preschool children. Ophthalmology. 2012;119:138-44. http://dx.doi.org/10.1016/j.ophtha.2011.06.024
14. Borchert M, Tarczy-Hornoch K, Cotter SA, Liu N, Azen SP, Varma R. Anisometropia in hispanic and african american infants and young children the multi-ethnic pediatric eye disease study. Ophthalmology. 2010;117(1):148-53. http://dx.doi.org/10.1016/j.ophtha.2009.06.008
15. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of myopia and hyperopia in 6 to 72-month-old african american and hispanic children: the multi-ethnic pediatric eye disease study. Ophthalmology. 2010;117:140-7. http://dx.doi.org/10.1016/j.ophtha.2009.06.009
16. Fozailoff A, Tarczy-Hornoch K, Cotter S, Wen G, Lin J, Borchert M, Azen S, Varma R. Prevalence of astigmatism in 6 to 72-month-old african american and hispanic children: the multi-ethnic pediatric eye disease study. Ophthalmology. 2011;118:284-93. http://dx.doi.org/10.1016/j.ophtha.2010.06.038
17. Colburn JD, Morrison DG, Estes RL, Li C, Lu P, Donahue SP. Longitudinal follow-up of hypermetropic children identified during preschool vision screening. J AAPOS. 2010;14;211-5. http://dx.doi.org/10.1016/j.jaapos.2010.02.006
18. Donahue SP. Relationship between anisometropia, patient age, and development of amblyopia. Am J Ophthalmol. 2006;142:132-40. http://dx.doi.org/10.1016/j.ajo.2006.02.040
19. Leon A, Donahue SP, Morrison DG, Estes RL, Li C. The age-dependent effect of anisometropia magnitude on anisometropicamblyopia severity. J AAPOS. 2008;12:150-6. http://dx.doi.org/10.1016/j.jaapos.2007.10.003


Funding source: None
Conflicts of interest: None
Received on:
December 16, 2016.
Reviewed in:
March 31, 2017.
Accepted on:
December 16, 2016.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados




 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket