

Ingrid de Oliveira Haubert Magalhães1; Renata Cavalcante Girão2; Francisco Saulo Sampaio Cardoso Tavares2; Keila Miriam Monteiro de Carvalho3
DOI: 10.17545/eOftalmo/2021.0004
ABSTRACT
OBJECTIVE: To perform a literature review on the use of protective eyewear in sports and its correlation with sports-related eye injuries.
METHODS: We searched the PUBMED database using keywords, such as protective eyewear, protective lenses, sports, injury in athletes, eye trauma, and special glasses. Following this, we performed a literature review of eye injuries in sports using the selected articles, with a focus on the use of protective eyewear.
RESULTS: We found 54 articles on the use of protective eyewear in sports up to 2018. They included a variety of sports and most of the injuries were blunt trauma caused by an object (usually a ball), of varying sizes, or direct trauma to the eye caused by a body part and/or a racquet. This report compiles data regarding these injuries to present an analysis of the topic in literature.
CONCLUSION: Sports-related eye injuries account for a large proportion of the care provided by ophthalmologists, thus having a potential impact on healthcare. Herein, we reiterate the importance of raising awareness among health professionals, such as ophthalmologists and pediatricians, as well as educators, about the use of eye protection in sports. This is primarily essential for ensuring the correct prescription of eyewear and for raising awareness among patients and guardians about the importance of its use.
Keywords: Protective eyewear; Protective lenses; eye trauma, Sports; Eye injury; Low vision; Blindness.
RESUMO
OBJETIVO: Realizar uma revisão na literatura sobre o uso de óculos de proteção nos esportes e correlacionar com os traumas oculares oriundos da prática esportiva.
MÉTODOS: Pesquisa na base de dados PUBMED com as palavras-chave: óculos de proteção, lentes de proteção, esportes, traumatismos em atletas, trauma ocular e óculos especiais. Dos artigos encontrados, foi realizada uma revisão de trauma ocular nos esportes, com relação ao uso e não uso de óculos de proteção.
RESULTADOS: Foram encontrados 54 artigos sobre lentes de proteção ocular nos esportes até o ano de 2018. Os esportes foram diversificados, sendo que a maioria dos traumas foram contusos, através de um objeto (geralmente bola), de variados tamanhos, ou trauma direto ao olho com partes do corpo e/ou raquetes. Este artigo apresenta através de uma compilação desses dados uma análise do tema na literatura.
CONCLUSÃO: As lesões esportivas oculares são responsáveis por uma grande proporção de atendimentos oftalmológicos, com potencial impacto na prestação de serviços. Reitera-se a importância da conscientização de profissionais de saúde como oftalmologistas e pediatras, assim como de educadores sobre o uso da proteção ocular na prática de esportes, para que se faça uma prescrição correta e alerte ao paciente e responsáveis sobre a importância do uso.
Palavras-chave: Óculos de proteção; Lentes de proteção; Trauma ocular; Esportes; lesão ocular; Baixa visão; Cegueira.
INTRODUCTION
Sports injuries account for more than 100,000 avoidable eye injuries every year. Protective eyewear (such as special glasses and helmets), reduce the risk of eye injury by about 90% as long as they fit correctly1,2.
To determine the degree of eye protection that is required for a specific sport or activity, one should consider whether there is a risk of small particles, projectiles, or objects reaching the eyes, or a risk of substances damaging the eye surface through contact or dispersion of environmental pollutants3.
It is recommended that every person should constantly be alert toward the possibility of potential accidents, especially around children and adolescents as they are a high-risk group for eye injuries in sports4.
The American Academy of Pediatrics and the American Academy of Ophthalmology consider the use of protective eyewear mandatory for all functionally monocular individuals and athletes who have undergone eye surgery or have eye diseases requiring special protection, such as high myopia5.
Alarming signs and symptoms warranting referral to the ophthalmologist
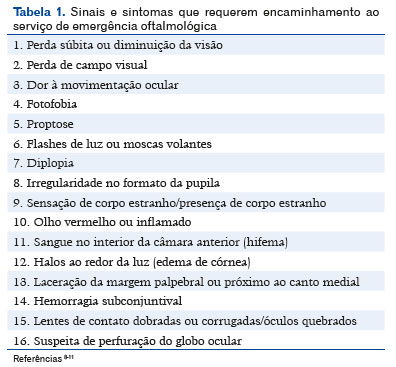
Considering the various mechanisms of trauma, the possibility of increased severity, and the importance of early treatment, some alarming signs and symptoms should be recognized as soon as possible (Table 1). If they are present, the patient should be referred to the ophthalmic emergency service6,7. This information should be disseminated beyond just medical professionals and is extremely important for education professionals (especially physical education teachers and coaches).
METHODS
This review sought to correlate the use of protective eyewear in sports and sports-related eye injuries, as well as evaluate the specific types of lenses used in each sport and the classification of sports-related risk. The references were obtained from the PUBMED database. The Portuguese and English keywords used included protective eyewear, protective lenses, sports, injury in athletes, eye trauma, and special glasses. The search yielded 54 articles on the topic. The patients differed in age, sex, and ethnicity. The inclusion criteria for the review were articles correlating physical activity, eye injury, and the use of protective eyewear in sports. We excluded case reports of trauma that were not sports related, studies that did not address the use of eyewear or protectors in sports, and studies that solely investigated the players’ acceptance of the use of protective eyewear.
RESULTS
The search yielded 54 articles. Case reports of trauma that were not sports related, studies that did not address the use of eyewear or protectors in sports, and studies that solely investigated the players’ acceptance of the use of protective eyewear were excluded from the review.
Several studies have shown a change in the scenario of this condition. Injuries are occurring more frequently in recreational and sports activities and are 2-3 times more likely to occur in outdoor environments12,13. The use of protective eyewear with sturdy plastic material and a safe design has been advocated14-16.
The use of eyewear was deemed as a direct cause of eye injury in only a few articles, which did not mention the material of the lenses. The vast majority of studies strongly advocate wearing protective eyewear during sports practice to prevent eye injuries.
In a study conducted by Pieper, patients were encouraged to try wearing protective eyewear that met the safety requirements established for each sport until they found eyewear that was comfortable and fit perfectly. In addition, patients were informed that the sensation of impaired vision caused by the bars on the protective eyewear worn in some sports would probably disappear with time17.
Ong et al. conducted a study in an ophthalmological hospital in the city of London between May and July 2008 to investigate the role of protective eyewear in the prevention of sports-related eye injuries. Despite the short study period (3 months), 48 patients with sports-related eye injuries were identified. Of these, 14 (29.2%) had 1 eye lesion, 18 (37.5%) suffered 2 eye lesions, and 10 (20.8%) had >2 eye lesions. Sixteen patients (33.3%) suffered trauma to the anterior and posterior segments. One patient (2%) was wearing prescription glasses (the material of the lenses was not mentioned), whose lenses shattered when hit by a shuttlecock, resulting in a penetrating injury. All patients (100%) were injured in only 1 eye. No patient wore eye protection or received advice on the prevention of future injuries, according to records18.
Moon et al. conducted a study correlating eye injuries and sports and concluded that lesions were more common in patients aged <10 years and that the rate of protective eyewear use was lower among these patients. This rate was also low among adults and their injuries commonly occurred during walking. The authors suggest that athletes should be educated and supplied with protective eyewear, and that a policy for the use of protective equipment should be implemented19.
Parver et al. conducted a study from 1985 to 1991 in which they observed that glass or plastic were reported as the cause of trauma in 2.9% of cases of eye injuries occurring in individuals who wore eyewear, which suggests that the broken lens contributed to the lesion14.
Christianson et al. conducted a retrospective study from 1967 to 1977 and detected 446 penetrating eye injuries. They attributed 16 of them to the use of eyewear (unspecified material)16.
In a study conducted in 2015 by Kriz et al., it was confirmed that a national mandate for protective eyewear to be worn by girls participating in field hockey in the US was associated with a 3-fold reduction in the rate of ocular/orbital injuries, without significantly increasing the frequency of player-to-player head or face contact and lesions, including concussion20.
Bro and Ghosh conducted a study in Sweden and reported that only 1 of 98 patients with eye injury caused during floorball had worn protective eyewear at the time of injury. Sixty-eight percent of players registered in the Swedish Floorball Federation stated that protective eyewear is required for players <15 years of age. Injuries among registered players are unusual, which indicates that this requirement is effective in eye protection21. In another study conducted in Finland by Leivo, Puusaari, and Mäkitie (2007), only a small percentage of floorball players wore protective eyewear22. In 2015, compared to the previous study, Leivo, Haavisto, and Sahraravand showed that eye injuries in floorball decreased significantly, mainly due to mandatory use of protective eyewear for younger players, and recommended that it becomes mandatory for all ages23.
Micieli, Zurakowski, and Ahmed, in a study published in 2014, showed that the individual risk of eye or orbital injury is significantly increased in players who choose not to use a visor in hockey24.
In a retrospective study conducted in Austria by Weitgasser, Wackernagel, and Oetsch on patients with golf-related eye injuries and who had been hospitalized for ophthalmic treatment between 1993 and 2000, 3 individuals had closed-eye injury and 4 had eyeball rupture. All patients required surgery, with the resulting visual acuity ranging from hand motion to 20/20. Three eyes required enucleation. Given the serious complications resulting from golf-related eye injuries, the authors believe that eye protection should be considered and promoted25. The authors Goldstein and Wee26 and Napier et al.27 recommended not wearing regular glasses during sports activities due to their propensity to shatter and cause additional injuries, especially during sports involving projectiles. In a study conducted by Crane et al., it was observed that the rate of eye injuries in golf was significantly lower among individuals who did not wear glasses than among those who wore glasses or sunglasses. This may be due to sunglasses and glasses protecting against minor injuries and the golfer not seeking subsequent care, or it may be more likely due to eye damage caused by sunglasses or glasses. It is recommended that golfers who wear sunglasses consider using glasses that conform to the American Society for Testing and Materials (ASTM) F803 standard28. With regard to cricket, authors Mann and Dain suggest considering a change in regulations to encourage the use of appropriate safety measures and personal eye protection by wicket-keepers29,30. Paintball is another sport associated with significant risk of severe eye injuries31,32. Standard practice procedures for paintball have been established by the ASTM, which specify minimum safety requirements, such as eye, ear, and face protection. Most of the reported injuries occurred while the athletes were not wearing protectors. Fogging up of lenses was 1 of the reasons why players removed them31.
With regard to squash, there are publications since 1978 advocating that healthcare professionals should be responsible for encouraging players to play squash with adequate eye protection33.
Lacrosse is another sport that is commonly associated with eye injury. Injuries occur at all levels of the game, in many different situations, and by various mechanisms. Therefore, mandatory use of eyewear is necessary to avoid serious eye injuries, especially in women’s lacrosse34.
DISCUSSION
Mechanisms of injury in sport
There are several mechanisms of eye injury, such as open-eye injury and closed-eye injury35, the most common in sports being closed-eye injury36.
The severity of the trauma will depend on the speed, force, and size of the object when it hits the eye. Objects smaller than the eyeball (<5cm) tend to compress the anterior segment of the eye, which distends medially, and increase the pressure on the intraocular structures, whereas objects larger than the eyeball (>5cm) increase the pressure on the floor or medial side of the eyeball, causing bone injury37.
Traumatic optic neuropathy is a condition that may occur either by direct injury to the optic nerve fibers (by bone fragments, hematomas, or penetrating injury) or by indirect injury, that is, damage due to transmission of forces to the optic canal. It is common for funduscopy to appear normal in the acute phase and progress with optic atrophy 3-6 weeks after the injury36.
Risk classification in sports
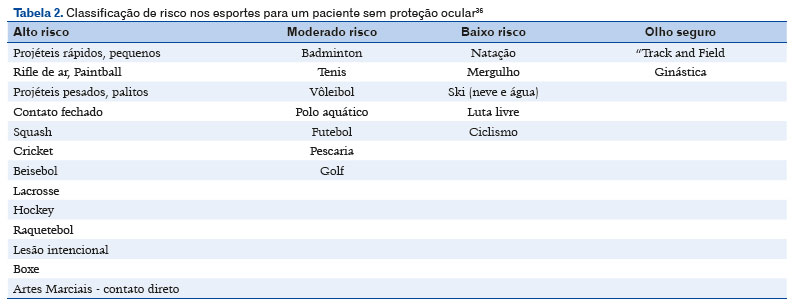
Sports can be classified according to their risk of causing eye injury, whether by collision, contact, or non-contact. They are classified into low-risk, moderate-risk or high-risk sports. In addition, some sports are considered safe for the eyes29,36 (Table 2).
Protective eyewear recommended for sports
The recommended eye protection for each sport is guided by the principle of energy absorption in a protective device that sits in front of the eyes (racket sports, baseball, and basketball). It should be determined by standards established by the ASTM5. Protective eyewear or glasses with UV protection should be worn during snow or water skiing. They help protect the eyes from sunburn and glare. Protective eyewear is often made of polycarbonate, a highly impact-resistant plastic capable of absorbing UV light. This plastic is 8 times stronger than other materials and is therefore preferred for use in protective eyewear. The impact resistance of normal glasses is only 4% to 5% that of polycarbonate of comparable thickness37.
Rimless glasses and smaller frames increase the risk of eye injuries38.
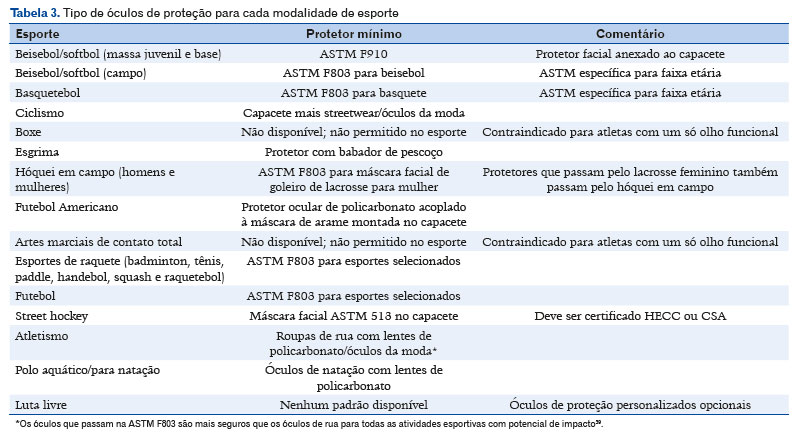
Below is the recommended protective eyewear for each sport (Table 3)39.
Impact and energy of the object
In addition to the choice of lens material, the structure and fit of the eyewear influence protection38. Most work-related eye injuries, despite the use of protective eyewear, are caused by objects coming from above, below, or the side of the protective eyewear39.
Examples of the impact and average energy of objects used in some sports in various countries across the world are shown below (Table 4).

Resistance of optical materials
Plastics are generally more resistant to impact than glass, especially to small, fast-moving objects. Polycarbonate is universally reported as the most impact-resistant eyewear lens material37.
There are several materials that can be used for eyewear frame manufacture, including polycarbonate and thermoplastic, which can incorporate foam coatings. These provide comfort and cushioning against any impact transferred to the eyeball27.
Patients with monocular vision and athletes with subnormal vision
Protective eyewear is mandatory for patients with low vision or monocular vision, as well as those who underwent ophthalmic or post-traumatic surgery40. Patients with subnormal vision, history of eye injury, monocular vision, or pre-existing eye disease (such as high myopia or retinal degeneration) should consult an ophthalmologist41 for assessment and guidance on the risks to vision arising from specific sports and long-term consequences that may affect the injury in the good eye42.
Eye protection in sports among children and young adults
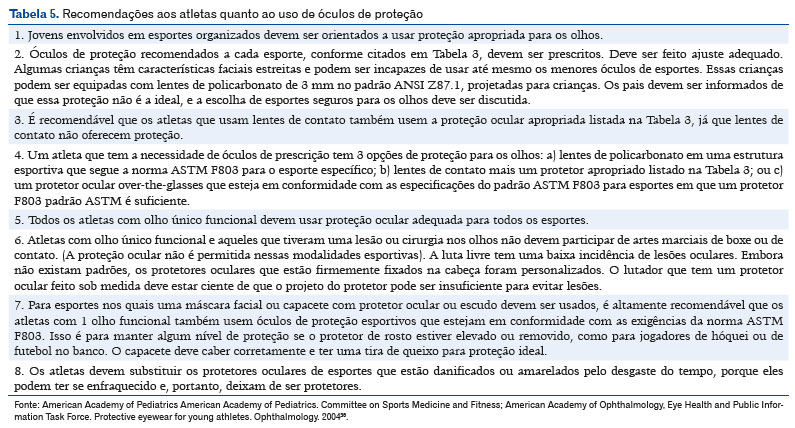
According to the American Academy of Pediatrics and the American Academy of Ophthalmology, it is highly recommended to use eye protection in sports that pose a risk of eye injury. The recommendations to be provided to athletes are shown in Table 540.
Sports-related eye injuries account for a large proportion of emergency eye care, with potential impact on care provision.
The recommended protective eyewear required for each sport is guided by the principle of energy absorption in a protective device that is placed in front of the eyes in sports that use a racket, bat, or ball, such as tennis, baseball, and basketball, respectively.
Considering the importance of preventing eye injury in sports, health professionals and educators should be made aware of the correct use of protective lenses in sports.
REFERENCES
1. Vinger PF. Sports eye injuries a preventable disease. Ophthalmology. 1981;88(2):108-13.
2. Larrison WI, Hersh PS, Kunzweiler T, Shingleton BJ. Sport-related ocular trauma. Ophthalmology. 1990;97(10):1265-9.
3. American Academy of Ophthalmology. Protective Eyewear. Disponível em: https://www.aao.org/eye-health/tips-prevention/injuries-protective-eyewear
4. Chen AJ, Chan JJ, Linakis JG, Mello MJ, Greenberg PB. Age and consumer product related eye injuries in the United States. R I Med J. 2014;97(1):44-8.
5. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Protective eyewear for young athletes. Pediatrics. 2004;113(3):619-22.
6. Mishra A, Verma AK. Sports related ocular injuries. Med J Armed Forces India. 2012;68(3):260-6.
7. Chb JG, Franzco APW, Franzco GW. Effects of Exercise on Ocular Physiology and Disease. Surv Ophthalmol. 2009;54(3):349-55.
8. Dain SJ. Materials for occupational eye protectors. Clin Exp Optom. 2012;95(2):129-39.
9. Hoskin AK, Philip S, Dain SJ, Mackey DA. Spectacle-related eye injuries, spectacle-impact performance and eye protection. Clin Exp Optom. 2015;98(3):203-9.
10. Flood L. Work-Related Eye Injuries in Australia. Canberra: Australian Government. Australian Safety and Compensation Council, 2008.
11. Protective Eyewear for young athletes. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics. 1996 Aug;98(2 Pt 1);311-3.
12. Cao H, Li L, Zhang M, Li H. Epidemiology of pediatric ocular trauma in the Chaoshan Region, China, 2001-2010. PLoS One. 2013;8(4):e60844.
13. MacEwen CJ, Baines PS, Desai P. Eye injuries in children: the current picture. Br J Ophthalmol. 1999;83(8):933-6.
14. Parver LM, Dannenberg AL, Blacklow B, Fowler CJ, Brechner RJ, Tiesch JM. Characteristics and causes of penetrating eye injuries reported to the National Eye Trauma System Registry, 1985-91. Public Health Rep. 1993;108(5):625-32.
15. Sinclair SA, Smith GA, Xiang H. Eyeglasses-related injuries treated in U.S. emergency departments in 2002-2003. Ophthalmic Epidemiol. 2006;13(1):23-30.
16. Christianson MD, Parker JA, Arndt J. Material and thickness: the important factors in the impact resistance of spectacle lenses. Can J Ophthalmol. 1977;12(4):300-3.
17. Pieper P. Epidemiology and Prevention of Sports-related Eye Injuries. Journal of emergency nursing: JEN: official publication of the Emergency Department Nurses Association. 2010. 36. 359-61. 10.1016/j.jen.2010.03.013.
18. Ong HS, Barsam A, Morris OC, Siriwardena D, Verma S. A survey of ocular sports trauma and the role of eye protection. Cont Lens Anterior Eye. 2012;35(6):285-7.
19. Moon S, Ryoo HW, Ahn JY, Park JB, Seo KS, Shin SD, et al. Analysis on sports and recreation activity-related eye injuries presenting to the Emergency Department. Int J Ophthalmol. 2016;9(10):1499-505.
20. Kriz PK, Zurakowski D, Almquist JL,Reynolds J, Ruggieri D, Collins CL, et al. Eye Protection and Risk of Eye Injuries in High School Field Hockey. Pediatrics. 2015;136(3):521-7.
21. Bro T, Ghosh F. Floorball-related eye injuries: The impact of protective eyewear. Scand J Med Sci Sports. 2017;27(4):430-4.
22. Leivo T, Puusaari I, Mäkitie T. Sports-related eye injuries: floorball endangers the eyes of young players. Scand J Med Sci Sports. 2007;17(5):556-63.
23. Leivo T, Haavisto AK, Sahraravand A. Sports-related eye injuries: the current picture. Acta Ophthalmol. 2015;93(3):224-31.
24. Micieli JA, Zurakowski D, Ahmed II. Impact of visors on eye and orbital injuries in the National Hockey League. Can J Ophthalmol. 2014;49(3):243-8.
25. Weitgasser U, Wackernagel W, Oetsch K. Visual outcome and ocular survival after sports related ocular trauma in playing golf. J Trauma. 2004;56(3):648-50.
26. Goldstein MH, Wee D. Sports injuries: an ounce of prevention and a pound of cure. Eye Contact Lens. 2011;37(3):160-163. doi:10.1097/ICL.0b013e31821790db
27. Napier SM, Baker RS, Sanford DG, Easterbrook M. Eye Injuries in Athletics and recreation. Surv Ophthalmol. 1996;41(3):229-44.
28. Crane ES, Kolomeyer AM, Kim E, Chu DS. Comprehensive Review of Golf-Related Ocular Injuries. Retina. 2016;36(7):1237-43.
29. Dain SJ. Sports eyewear protective standards. Clin Exp Optom. 2016;99(1):4-23.
30. Mann DL, Dain SJ. Serious eye injuries to cricket wicketkeepers: a call to consider protective eyewear. Br J Sports Med. 2013; 47(10):607-8.
31. Al-Amry M, Al-Ghadeer H. Paintball related ocular injuries: First case report in Saudi patients. Saudi J Ophthalmol. 2017;31(1):55-7.
32. Taban M, Taban M, Sears J. Ocular findings following trauma from paintball sports. Eye (Lond). 2008;22(7)930-4.
33. Easterbrook M. Eye injuries in squash: a preventable disease. Can Med Assoc J. 1978;118(3):298, 303-5.
34. Waicus KM, Smith BW. Eye Injuries in Women’s Lacrosse Players. Clin J Sport Med. 2002;12(1):24-9.
35. Rodriguez JO, Lavina AM, Agarwal A. Prevention and treatment of common eye injuries in sports. Am Fam Physician. 2003;67(7): 1481-8.
36. American Academy of Pediatrics, Committee on Sports Medicine and Fitness, American Academy of Ophthalmology, Eye Health and Public Information Task Force. Protective eyewear for young athletes. Ophthalmology. 2004;111(3):600-3.
37. Vinger PF, Duma SM, Crandall J. Baseball hardness as a risk factor for eye injuries. Arch Ophthalmol. 1999;117(3):354-8.
38. Erie JC. Eye Injuries: prevention, evaluation, and treatment. Phys Sportsmed. 1991;19(11):108-22.
39. Jeffers JB. Sports-related eye injuries. In: Mellion MB, ed. Sports Medicine secrets. 2d ed. Philadelphia: Hanley & Belfus, 1999: 243-7.
40. Tucker AM. Common soccer injuries. Diagnosis, treatment and rehabilitation. Sports Med. 1997;23(1):21-32.
41. Turrif TM, Gerali PS. Do not play game with your eyes. J Ophthalmic Nurs Technol. 1991;10(2):82-3.
42. Eye injuries and eye protection in sports. A position statement from the Internacional Federation of Sports Medicine (F.I.M.S.). Br J Sports Med. 1989;23(1):59-60.
AUTHOR’S INFORMATION


Funding: No specific financial support was available for this study
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose
Received on:
April 27, 2020.
Accepted on:
November 2, 2020.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket